MEDRADSC 3C03 Lecture Notes - Lecture 19: Cholangiography, Bile Duct, Endoscopic Retrograde Cholangiopancreatography

14 Jul 2018
School
Department
Course
Professor
Document Summary
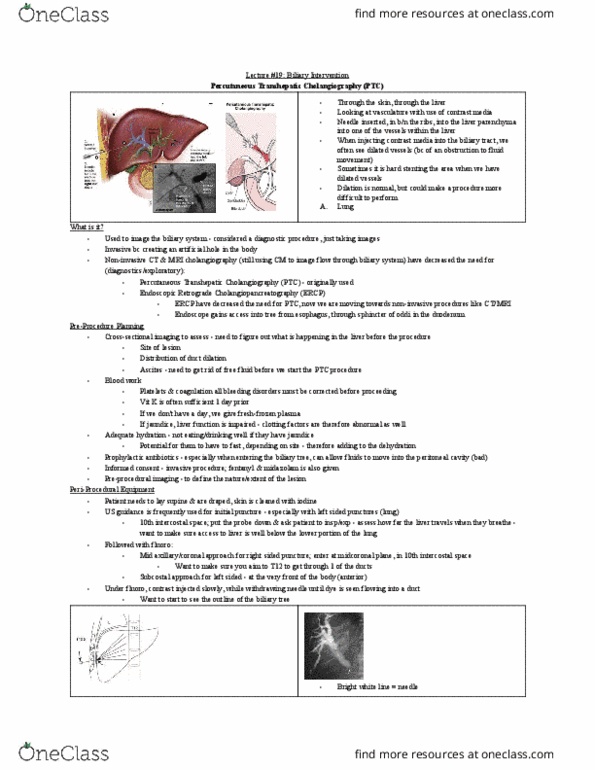
Percutaneous transhepatic cholangiography: trying to get it into the bile duct. Ptc is last resort: non-invasive ct / mri cholangiography / ercp have decreased the need for it. Cross-sectional imaging (ct or mri) to assess: site of lesion, nature/extent of lesion, distribution of duct dilation. Blood work: platelets and coagulation, all bleeding disorder must be corrected first (inr and ptt, vitamin k good 1 day prior. Us guidance for initial puncture (esp left sided punctures: mid axillary approach for right, subcostal approach for left under xyphoid o. Overall complications: a: resulting cholangiogram, not bright white (we expect it to be) . filling defects, they hit a blood vessel pseudoaneurysm. Failed endoscopic drainage that was performed from obstructive jaundice. Malignant disease of the bile ducts or pancreas. Imaging is used to assess: obstruction cause and extent, biliary anatomy. Modality: many factors define the best modality for insertion, often us immediately beforehand.