Pathology 3500 Lecture Notes - Lecture 31: Sepsis, Cardiac Output, Urinary Retention

28 Mar 2018
School
Department
Course
Professor
Document Summary
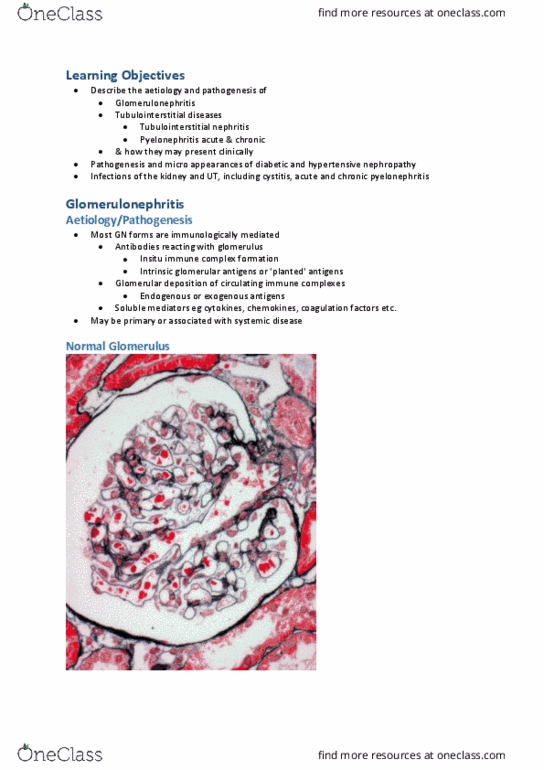
It ca(cid:374) get co(cid:373)plicated - (cid:449)o(cid:374)t put e(cid:373)phasis o(cid:374) this, do(cid:374)"t e(cid:448)e(cid:374) thi(cid:374)k (cid:449)e (cid:374)eed this list: minimal change disease. Focal segmental glomerulosclerosis: membranous glomerulopathy, diabetes mellitus, amyloidosis, post-infectious glomerulonephritis, membranoproliferative glomerulonephritis. Iga nephropathy: hereditary nephritis, rapidly progressive glomerulonephritis, anti-basement membrane disease (goodpasture"s syndrome, polyarteritis nodosa, microscopic polyarteritis, wegener"s granulomatosis, henoch schoenlein purpura, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome. Investigations: urinalysis, hematuria (blood in urine) - can get in bc filter isn"t working right, proteinuria (protein in urine, this is what is spilling into the urine, blood: Increased creatinine and urea (impaired waste elimination: kidney biopsy: - best way to figure out what is going on, needed for definitive diagnosis of glomerular diseases. Inflamed (glomerulonephritis) , too many cells , inflamm cells migrating in: thickened matrix, obscured capillaries. Immunofluorescence: throw in fluroescent tags and look for various compounds like igg, ige, iga etc.