NUR 4227 Study Guide - Final Guide: Intracranial Hemorrhage, Traumatic Brain Injury, Posterior Pituitary

Document Summary
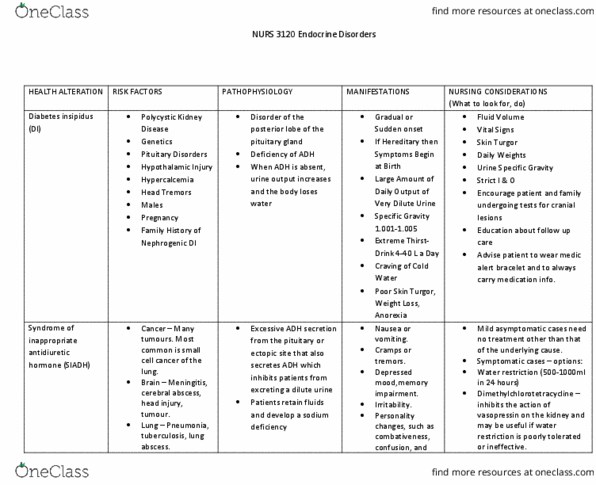
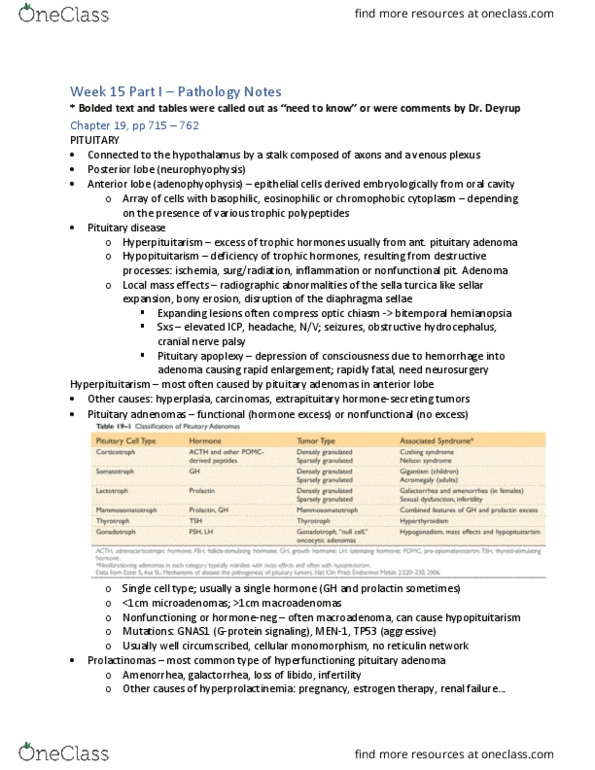
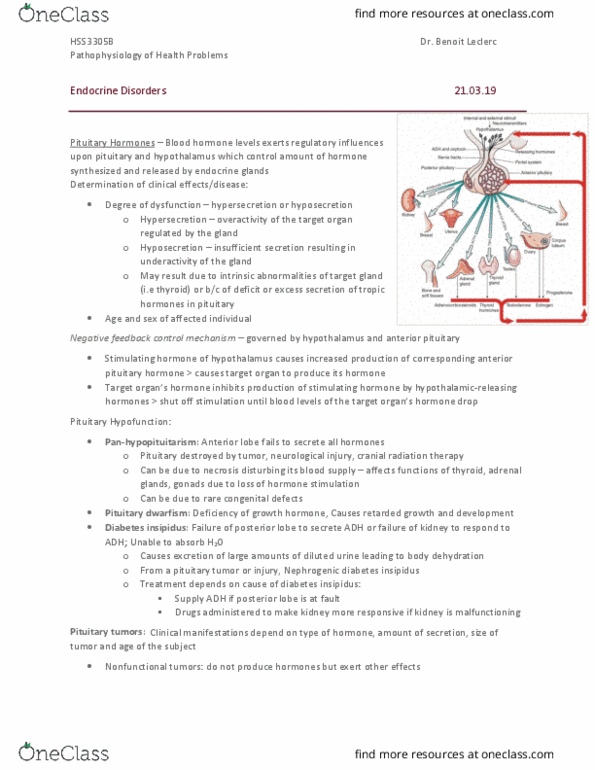
Module regulatory/endo: understand pathophysiology, causes, clinical manifestations, laboratory manifestations, clinical management and nursing care of individuals with: Di**: diabetes insipidus, water loss via renal system, limited water retention due to lack of adh, hypotonic (very dilute) urine. Excess fluid loss: transient, head trauma, permanent, cranial surgery, causes, hypothalamic injury, surgery, or ischemia, pituitary injury, surgery, or ischemia, traumatic brain injury, cns infection - meningitis, encephalitis, cerebrovascular disease, cerebral edema, radiation brain, cranial neoplasms. Intracranial hemorrhage: autoimmune, familial disease, post intracranial surgery, commonly present with triphasic pattern, acute, abrupt onset of polyuria. Lithium (20% will develop di: demeclocycline, amphotericin, methoxyflurane, gentamicin, colchicine. Structural lesion in thirst center: psychiatric issues, manifestations, polydipsia, d/t compensation, will become fatigued from nocturia, polyuria, uo (> 2l/day or more) Stage 1 acute stage - polyuria: adh impaired re: nerve shock. Stage 2 interphase- (day 2-14) - water retention: urine volume normalizes.