ADMS 3502 Chapter Notes - Chapter 3.2: Left Ventricular Hypertrophy, Diastolic Heart Failure, Pulmonary Valve

21 May 2020
School
Department
Course
Professor
Document Summary
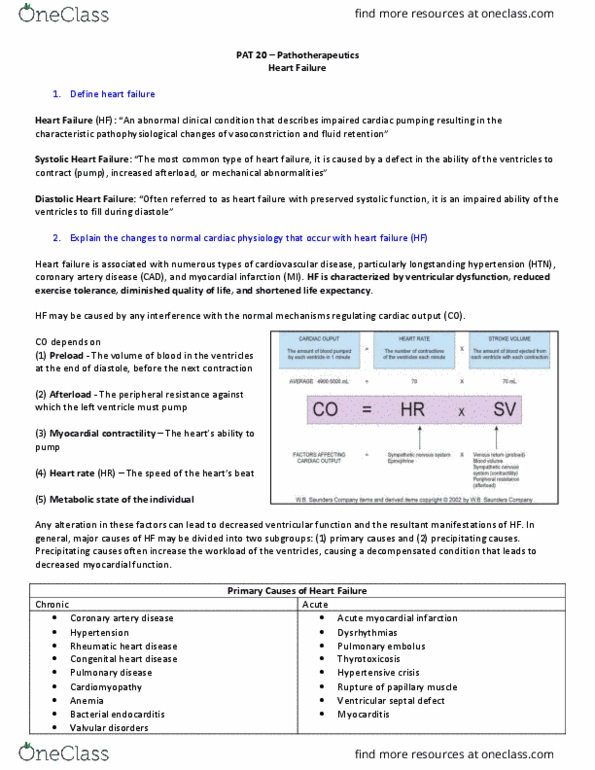
End-diastolic filling volumes dilate the heart = cardiac myofiber stretching = lengthened fibers contract more forcibly = cardiac output: compensated heart failure = dilated ventricle is able to maintain cardiac output. Neuro-endocrine systems activated: norepinephrine = hr, myocardial contractility, and vascular resistance, renin-angiotensin-aldosterone systems (raas) = circulatory volume and vascular tone, release of anf (or anp) These mechanisms have a limited ability to cope and ultimately cannot or are overwhelmed and fail. Rarer causes of chf: diastolic dysfunction = left ventricular hypertrophy, interstitial fibrosis (fibrosis = constrictive, interstitial infiltrates, pericardial disease. Chf mechanisms: connective tissue , result = interstitial heart disease , altered systolic and diastolic function. Complications of mi: sudden death = arrhythmias, acute heart failure, (transmural infarction, (subendocardial infarction, mural thrombosis, myocardial rupture, free wall. Iv septum: papillary muscle, left ventricular aneurysm/mural thrombus, chronic congestive heart failure, pericarditis.