PSL301H1 Study Guide - Midterm Guide: Dopamine Receptor, Limbic System, Chemoreceptor


RESPIRATORY SYSTEM
Overview of Function and Structure
Functions
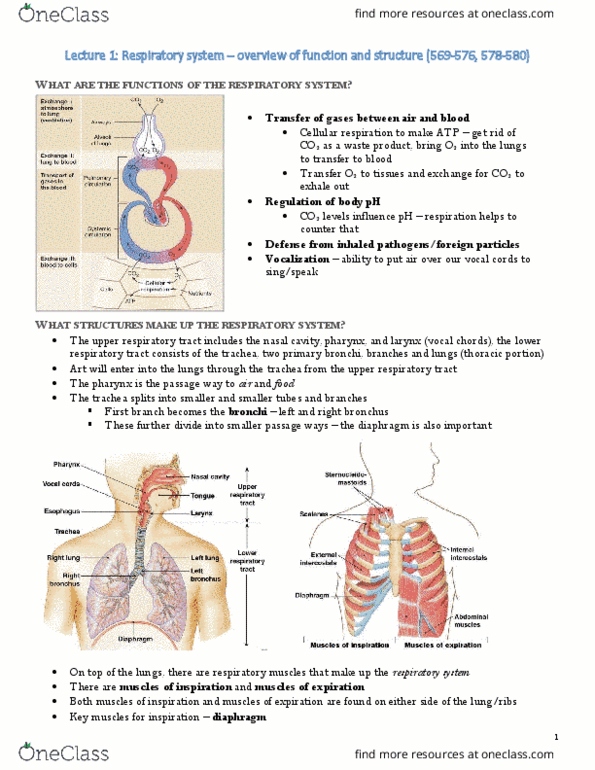
- transfer of ggases between air and blood
o O2 comes in → cellular respiration → ATP → CO2 expelled
- Regulation of body pH
o CO2 levels influence pH of the blood
- Defence from inhaled pathogens/foreign paricles
- Vocalization
o Air needed over vocal cords
Structures that make up Respiratory System
- pharynx (where both air and food pass)
- vocal cords
- trachea → bronchus
- diaphragm (needed for letting air in and out)
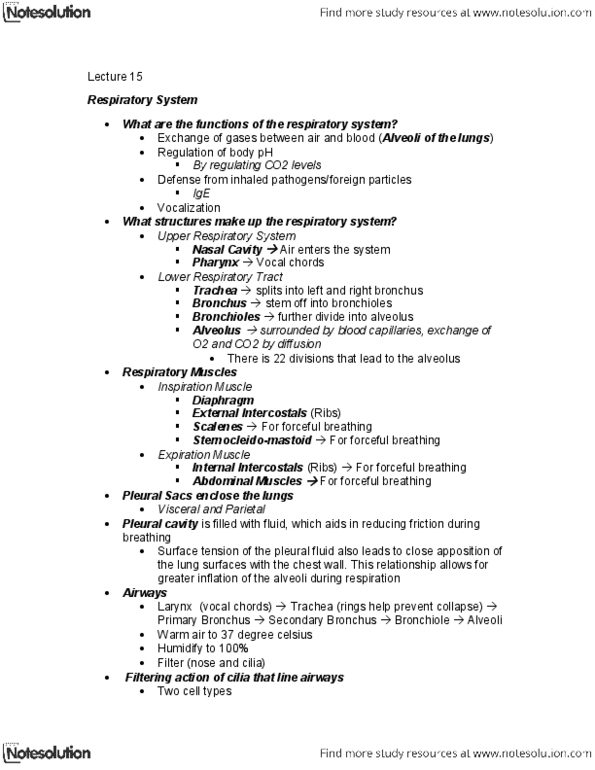
Respiratory Muscles
- muscles of inspiration:
o sternocleidomastoids – attach to the top
o scalenes – attach from top and to ribs
o external intercostals – in between ribs
o diaphragm – key muscle below rib cage
- muscles of expiration
o internal intercostals – has different orientation as the external ones
o abdominal muscles
Lungs
- pleural sacs enclose the lungs
- two pleural membranes and pericardial cavity in between
- the double membrane structure forms the ‘sac’
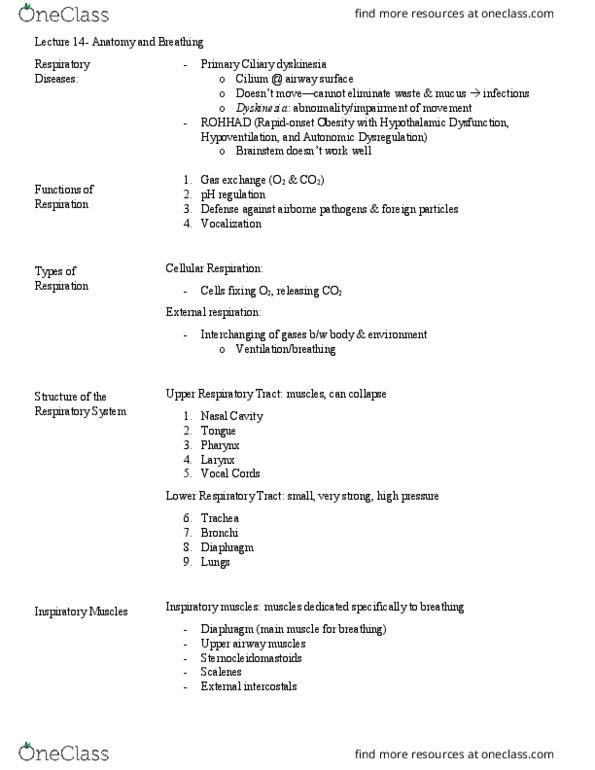
Airways
- air is relatively dry and cold, thus the pathway makes it get warmer and humidified
o air warmed to 37’C
o air humidified to 100%
o air filtered through nose and repspiratory cilia
- below larynx (voice cord) is trachea
- the trachea branches into two primary bronchi (left and right)
- primary bronchi then separates to secondary, and 22 more times terminating in a
cluster of alveoli
- filtering action of cilia – cilia beat in one direction and move the mucus to pharynx
side
- mucus layer traps inhaled particles. The particles then can be either coughed or
swallowed
o watery saline layer below mucus allow cilia to push mucus toward pharynx
- goblet cell secretes mucus
- immune cells along the epithelium also secrete antibodies to disable pathogens
o IgA
find more resources at oneclass.com
find more resources at oneclass.com

- Airway break down
o 1st bifurcation: right and left main bronchi
o 2~4th bifurcation: lobar bronchi
▪ Cartilage maintains their shape (and smooth muscle)
o 5~11th bifurcation: segmental bronchi
o 12~16th bifurcation: terminal bronchioles
▪ stabilized by bronchiolar smooth muscles
o all the above are “conducting airways” = no gas exchange
o constitute an anatomical dead space
▪ air in this region does not exchange anything with cells
Lobules
- Primary Lobule (and below): region of gas exchange
- Approximately 300 million alveoli, each about 300um in diameter
- Total cross-sectional area is very large, about 180cm squared, and air velocity is
virtually zero
- Alveoli are covered with rich blood supply (from pulmonary artery and then back to
heart in pulmonary vein)
- The exchange is between single layer of endothelial
- Type I alveolar cell
o Constitute the wall of the tissue
- Type II alveolar cell
o Produce surfactants → allow lungs expand more easily
- Elastic fibers constitute as part of the connective tissue
- Alveolar macrophages
o Engulf foreign particles
- Alveolar gas exchange occurs via by passive diffusion across endothelium
o Basement membranes are fused
Bloor transport to and from lungs
- 10% of the blood volume comes to lungs
- pressure is low: 25/8mmHg
- Heart (right ventricle) → pulmonary trunk → pulmonary arteries → pulmonary arterioles
→ capillaries (oxygenated) → pulmonary venules → pulmonary veins → heart (left
atrium)
- Pulmonary metarteriole have many branches of capillaries coming out
o In case of embolus / blockage, others will cover and filter
o Systemic capillaries on the other hand, serve a particular area, so when
blocked, the area gets killed
Defending respiratory system
- filtering action of nose
- mucous and action of cilia lining the airways
- antibodies secreted onto respiratory surfaces
- macrophages in respiratory tract including alveoli
Lung function → must see the wave diagram
- measured by Spirometry
find more resources at oneclass.com
find more resources at oneclass.com

o clinically used often (ex. before an operation)
o person breathes into a tube
o hollow cylinder sits on top water and moves up & down
o a pen detects the movement and detects change in volume
o usually change in volume is 0.5L
- Lung Volumes
o VT: tidal volume = normal change
o IRV: inspiratory reserve volume = the amount of air already in lung
o ERV: expiratory reserve volume = amount of air you can expel total
o RV: residual volume = amount of air that always stays in the lung
- Lung Capacity
o VC: vital capacity = inspiratory reserve volume + expiratory reserve volume +
tidal volume
o IC: inspiratory capacity = inspiratory reserve volume + tidal volume
o FRC: functional residual capacity = expiratory reserve volume + residual volume
o TLC: total lung capacity = inspiratory reserve volume + expiratory reserve
volume + residual volume + tidal volume
▪ Usually 7L avg male, 5L female
o Note: capacities are combinations of volumes, volumes are unique
- Different age & diseases can change lung volumes and capacities
o Young vs. Elderly
▪ Have similar IC
▪ Elderly has less ERV and more RV
o Obstructive lung disease – hard to get air out
▪ Emphysema – larger TLC
▪ Severe emphysema have upto 150% TLC of normal, and has large RV,
similar ERV
o Restrictive lung disease
▪ Have smaller TLC
▪ Pulmonary fibrosis – have difficulty expanding lungs
▪ Neuromuscular – large RV, and small ERV, due to difficulty moving air in &
out
▪ Severe Obesity – also have large RV, and small ERV due to ‘weighing
down by fat’
- Forced expiratory volume and vital capacity is when one is told to breath out as fast
as you can following maximal inhalation
o Forced expiratory volume (FEV) = volume of air forcefully exhaled in 1st second
o Forced vital capacity (FVC) = volume of air forcefully exhaled
o Normally, FEV = 3.6L, FVC = 4.5L
o FEV/FVC = 80%
o In case of restrictive lung disease, the ratio is approximately same, but the total
volume of exhale is less
o In case of obstructive…? Below
Case study
- John has asthma (obstructive)
- Structures affected = bronchioles, which narrow
- In a lung function test like FEV/FVC, the ratio would only be around 40%
find more resources at oneclass.com
find more resources at oneclass.com


41
PSL301H1 Full Course Notes
Verified Note
41 documents
Document Summary
Functions transfer of ggases between air and blood: o2 comes in cellular respiration atp co2 expelled. Regulation of body ph: co2 levels influence ph of the blood. Vocalization: air needed over vocal cords. Pharynx (where both air and food pass) Diaphragm (needed for letting air in and out) trachea bronchus. Muscles of inspiration: sternocleidomastoids attach to the top, scalenes attach from top and to ribs, external intercostals in between ribs, diaphragm key muscle below rib cage. Muscles of expiration: abdominal muscles internal intercostals has different orientation as the external ones. Pleural sacs enclose the lungs two pleural membranes and pericardial cavity in between the double membrane structure forms the sac". Air is relatively dry and cold, thus the pathway makes it get warmer and humidified: air warmed to 37"c, air humidified to 100, air filtered through nose and repspiratory cilia.