PATH 200 Study Guide - Midterm Guide: Small-Cell Carcinoma, Plasma Osmolality, Syndrome Of Inappropriate Antidiuretic Hormone Secretion

Document Summary
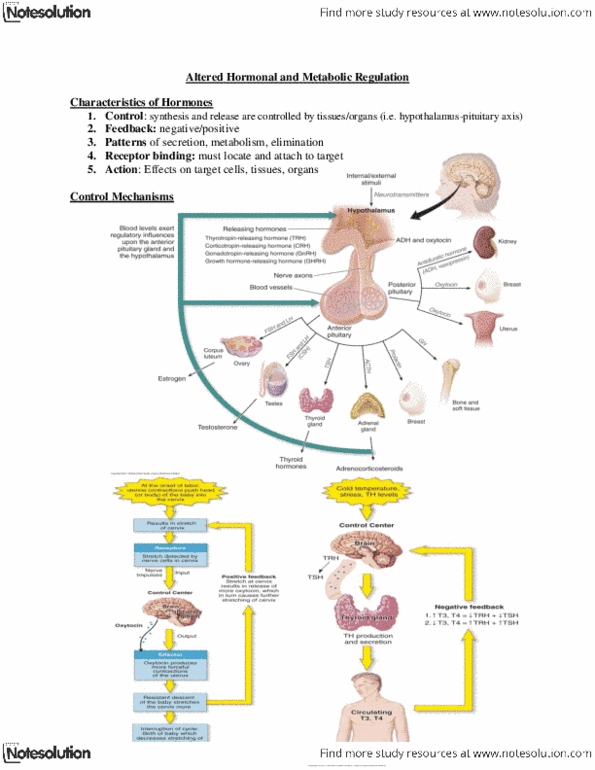
Hormone levels usually altered by: hyper- or hypoactivity of an endocrine gland failure of feedback systems damaged target tissues, or impaired receptors production of a hormone by non-endocrine tissue (ie. tumor - paraneoplastic syndrome) ~75% due to ectopic production of adh by tumor cells ie. small cell carcinoma of lung. Some cases siadh is the first indication of cancer. Inadequate response of renal tubules to adh due to lesions in collecting tubules. Sodiu(cid:373) (cid:894)h(cid:455)per(cid:374)atre(cid:373)ia(cid:895), osmolarity/ plasma osmolality (cid:894)h(cid:455)peros(cid:373)olarit(cid:455)(cid:895) thirst. Uri(cid:374)e output (cid:894)pol(cid:455)uria >12l/day), dilute and watery urine very thirsty (polydipsia) rapid dehydration, circulatory collapse nocturnia (need to wake to urinate) enlarged bladder, hydronephrosis (swollen kidney in long-standing disease) Normal adrenal function (produces aldostero(cid:374)e sti(cid:373)ulates na retention) Absence of other conditions that might alter fluid status. Correct any underlying cause (radiation therapy for tumor?) Hypertonic saline for emergency correction of severe hyponatremia. *acute hyponatremia can cause death from cerebral edema and brain stem herniation.