NURS 443 Lecture Notes - Lecture 5: Malaria, Vasopressin, Blood Pressure


Metabolism & Nutrition
Book Notes
A. Liver Failure
a. Definition: clinical syndrome characterized by severe impairment of liver function
associated w/ hepatic encephalopathy.
b. Cause:
i. drugs, cirrhosis, nonalcoholic fatty liver disease, biliary disease,
acetaminophen, alcohol, hepatitis A, B, or C (C affects the liver the most), liver
cancer, Malaria, Iatrogenic (caused by therapy such as steroids, meds, etc)
c. Risk factors: drug abuse, alcoholism, chronic NSAID use, chronic infection
d. Complications:
i. Ascites- accumulation of serous fluid in peritoneal or abd. Cavity
ii. encephalopathy- excessive ammonia and bilirubin levels cause neuroc
change
iii. portal hypertension- increase venous pressure in portal circulation
iv. gastric varices- complex of tortuous veins at lower end of esophagus,
which are enlarged and swollen
v. hepatorenal syndrome- type of renal failure w/ advancing azotempia,
oliguria, and intractable ascites
e. S&S: edema, ascites, bleeding/bruising, esophageal varices, malnutrition,
f. Treatment: liver transplant is treatment of choice
g. Interventions (look at cirrhosis)
i. Provide plenty of water, monitor glucose, and acid-base balance
ii. Avoid straining by providing stool softeners and monitor ICP
iii. Pad bed to avoid damage from seizures, avoid injury
iv. Monitor I&Os
v. Enteral nutrition may be necessary
vi. Avoid the use of barbiturates, sedative, hypnotics, acetaminophen, alcohol
B. Cirrhosis
a. Definition:
i. Chronic progressive disease of the liver characterized by extensive
degeneration and destruction of liver cells
b. Cause:
i. Chronic hepatitis C infection, alcoholism, protein malnutrition, genetics,
chronic inflammation, right-sided heart failure
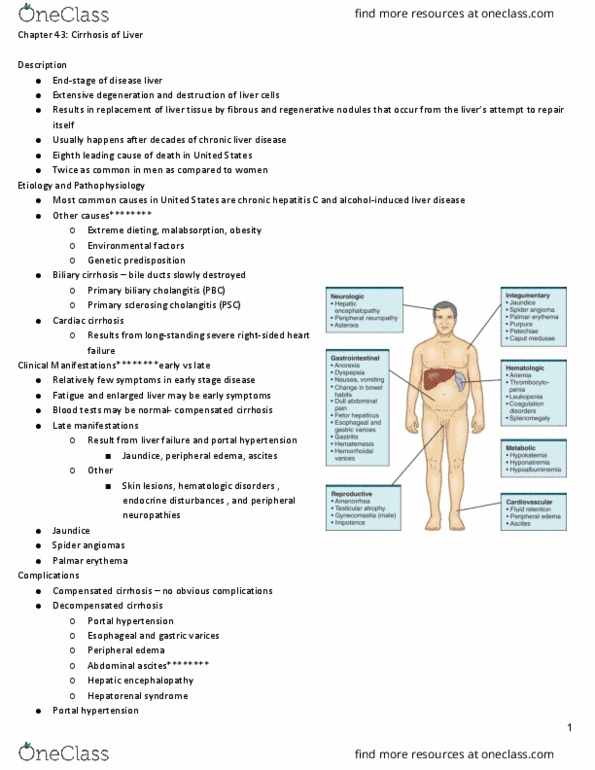
c. S&S
i. Early: insidious and include fatigue and may not be discovered until later
ii. Later: jaundice, peripheral edema, ascites, peripheral neuropathy, pain in RUQ
1. skin lesions (spider angiomas- spider veins)(palmar erythema(red
area that blanches w/ pressure),
2. hematologic disorder: thrombocytopenia, leukopenia, anemia, and
coagulation disorders
a. may not see these initially due to hemoconcentration
3. endocrine disturbances: gynecomastia in males, loss of axillary and
pubic hair, testicular atrophy, libido
d. Diagnosis
find more resources at oneclass.com
find more resources at oneclass.com

i. AST, ALT, total protein, decreased albumin, increased bilirubin, increased
globulin levels, decreased cholesterol, prolonged prothrombin time
e. Treatment
i. Paracentesis may be necessary if ascites occurs
ii. Balloon tamponade- used in treatment for hemorrhage
iii. Will typically have an upper endoscopy to screen for varices
iv. Trans jugular intrahepatic portosystemic shunt (TIPS) is placed to redirect
portal blood flow.
f. Interventions
i. Management of sodium restriction, diuretics, and fluid remove is key in
fixing ascites.
1. Albumin may be given to help maintain intravascular volume and
adequate urine output by increasing plasma colloid osmotic
pressure
2. Spironalctone (Aldactone) & Furosemide (Lasix)
a. Aldactone is potassium-sparing diuretic
ii. Stress the importance of avoiding alcohol, aspirin, and NSAIDS
iii. If arieal leed ours…
1. Manage the airway, IV therapy is initiated, provide blood
2. Octreotide(Sandostatin) or vasopressin may be given
a. Nitroglycerin is given hand in hand w/ vasopressin due to
risk of dysrhythmias, increased BP, and low coronary blood
flow
iv. Nutritional therapy
1. High calorie diet (3000cal/ day), high carb, low/moderate fat.
a. Protein may be restricted to 60g if patient has episodic
hepatic encephalopathy but not if persistent
encephalopathy
2. Enteral or parenteral nutrition may be necessary
3. Low sodium diet is necessary if pt. has edema or ascites
a. Limit to 2g/day but if sever should be 250- 500 mg/day
b. Inform to avoid canned foods, frozen foods, salted
snacks(potato chips), nuts, smoked meats, fish, crackers,
breads, olives, pickles, ketchup, and beer
4. Only restrict fluids to 1500ml/day if severe ascites
5. Provide oral hygiene before meals and allow for between-meal snacks
6. Vitamin and mineral supplement will be provided
C. Pancreatitis
a. Definition: inflammation of the pancreas
i. More common in men and middle aged adults
b. Acute vs. chronic pancreatic
i. Acute: Auto-digestion of glands(premature activation of trypsin begins
digesting pancreas)
ii. Chronic: will typically see weight loss, steatorrhea, mild jaundice w/ dark urine
c. Complications:
i. Pseudocyst & Abscess
1. Cavity continuous w/ normal function and pancreas fills w/ necrotic
products and liquid secretion
find more resources at oneclass.com
find more resources at oneclass.com