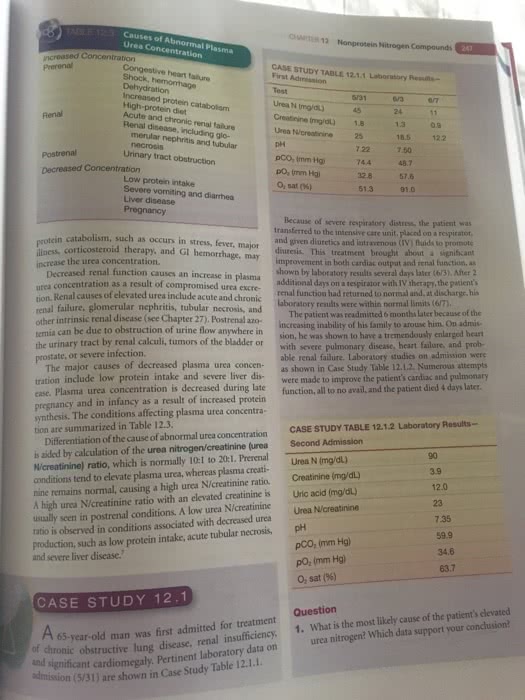
Causes of Abnormal Plasma Urea Concentration HAPTER 12 Nonprotein Nitrogen Compounds Congestive heart falure Shock, hemorrhage Dehydration Increased protein cataboliom High-protein diet Acute and chronic renal failure Renal disease, including glo- CASE STUDY TABLE 12.1.1 Laboratory Reis- First Admission Urea N (Img/d) Creatinine (mg/dl) 1.8 13 Urea N/creatinine 25 Renal merular nephritis and tubular 18.5 122 7.50 48.7 Urinary tract obstruction 744 Decreased Concentration Low protein intake Severe vomiting and diarrhea Liver disease pO, (mm Hg o,sat (%) 328 576 51.391.0 protein cin catabolism, such as occurs in stress, fever, major diuresis. This treatment brought about a illness, corticosteroid Because of severe respiratory distress, the patient was transferred to the intensive care unit, placed on a respirator and given diuretics and intravenous (IV) fluids to promote d therapy, and Gl hemorrhage, may signiÅicamt increase the urea concentration. Decreased urea concentration as a result of compromised urea excre- ed renal function causes an increase in plasma improvement in both cardiac output and renal function. as shown by laboratory results several days later (6/3).After 2 additional days on a respirator with IV therapy, the patik of elevated urea include acute anbere within normal limits (67), renal function had returned to normal and, at discharge, his dmitted 6 months later because of intrinsic renal disease (see Chapter 27). Postrenala temia can be due to obstruction of urine flow anywhere in the urinary tract by renal calculi, tumors of the bladder or prostate, or severe infection. increasing inability of his family to arouse him. On admis sion, he was shown to have a tremendously enlarged heart with severe pulmonary disease, heart failure, and prob- able renal failure. Laboratory studies on admission were The major causes of decreased plasma urea concen- as shown in Case Study Table 12.1.2. Numerous attempts tration include low protein intake and severe liver dis- were made to improve the patient's cardiac and pulmonary ease. Plasma urea concentration is decreased during late f pregnancy and in infancy as a result of increased protein synthesis. The conditions affecting plasma urea concentra function, all to no avail, and the patient died 4 days later Differentiation of the cause of abnormal urea concentration CASE STUDY TABLE 12.1.2 Laboratory Results is aided by calculation of the urea nitrogen/creatinine (urea Second Admission N/creatinine) ratio, which is normally 10:1 to 20:1. Prerenal conditions tend to elevate plasma urea, whereas plasma creati- nine remains normal, causing a high urea N/creatinine ratio. A high urea N/creatinine ratio with an elevated creatinine is Uric acid (mg/dl) usually seen in postrenal conditions. A low urea N/creatinine Urea N/creatinine ratio is observed in conditions associated with decreased urea production, such as low protein intake, acute tubular necrosis, pH tion are summarized in Table 12.3. 90 Urea N (mg/dl) 3.9 12.0 23 7.35 59.9 pCO: (mm Hg) pO, (mm Hg) O, sat (96) 34.6 and severe liver disease. 63.7 CASE STUDY 12.1 e chronic obstructive lung disease, renal insufficiency, 1. What is the most likely cause of the patient's clevated and 65-year-old man was first admitted for treatment urea nitrogen? Which data support your conclusion t laboratory data on au significant cardiomegaly. Pertinent (5/31) are shown in Case Study Table 12.1.1.