Physiology 3120 Lecture Notes - Lecture 55: Diabetes Mellitus Type 1, Diabetes Mellitus Type 2, Insulin Receptor

2 May 2018
School
Department
Course
Professor

Human Physiology Lecture 55
Diabetes and insulin resistance
- Type 2 diabetes: insulin receptor is impaired
- Type 1 diabetes: lack of insulin production
o Do not have beta cells to make insulin
o Organs do not have insulin to bind to its receptor to lower blood glucose
- Secondary issue of diabetes: eyesight, kidney failure, lack of circulation and lose limbs
o Quality of life
Diabetes Mellitus
- Diabetes—Greek--large volume of urine
o Have more urine secretion in diabetes patients
- Mellitus—Latin--a sweet taste.
- A lot of urine – with high glucose
o High filtration and excretion of the kidngeys to excrete that water and sugars in the urine
- The ancient Indians tested for diabetes by observing whether ants were attracted to a person's urine,
and called the ailment "sweet urine disease" (Madhumeha). The Korean, Chinese, and Japanese
words for diabetes also mean "sweet urine disease".
- Characterized by:
o Hyperglycemia
▪ High circulating blood glucose
o Polyphagia (eating with weight loss)
o Polyuria (high urine volume)
o Glycosuria (glucose in urine)
o Water and electrolyte loss
▪ Dehydration
o More of type 1, but also type two diabetes
- In severe cases (if not treated):
o Ketosis (high ketones)
▪ Poisonous to the cell and organism
o Acidosis
o Coma and death
▪ Long term
- Long-term complications: retinopathy (impaired vision), nephropathy (impaired kidney function),
angiopathy (blood clots – lead to amputations of organs), and increased susceptibility to infection
o Secondary conditions, even if they control blood glucose, the long term complications can
still occur
- Type I
o Insulin-dependent
▪ Total lack of insulin being produced. Do not have the beta cells that are making
insulin to support the needs of the body to lower blood glucose
o Autoimmune destruction of pancreatic cells
▪ Autoimmune disease
o Early onset juvenile diabetes
▪ Children and adolescents (usually diagnosed in HS)
o ~10% of diabetics
find more resources at oneclass.com
find more resources at oneclass.com

- Type II
o Insulin resistant/impaired insulin secretion
▪ Have insulin BUT are not responding to the insulin, when insulin binds to receptor
there is an impaired response
▪ RECEPTOR IS NOT WORKING
o lifestyle-overweight, sedentary
▪ Lack of activity
o Onset in mid-life
▪ Occurs alter in life (30,40,50 years of age)
▪ With epidemic of childhood obesity, the rate of Type 2 diabetes shifting, and
occurring in a younger population
o 90% of diabetics
Type I Diabetes
- A failure to secrete sufficient insulin to regulate glucose utilization
- Autoimmune disease
o Bodys immune system believes the beta cells are foreign
o T cells from the thymus attack the beta cells and destroy them
- ~ 10% of all diabetes; early onset
- Insulin-dependent
- Early symptoms: high glucose in urine, dehydration, low energy
o High urine output
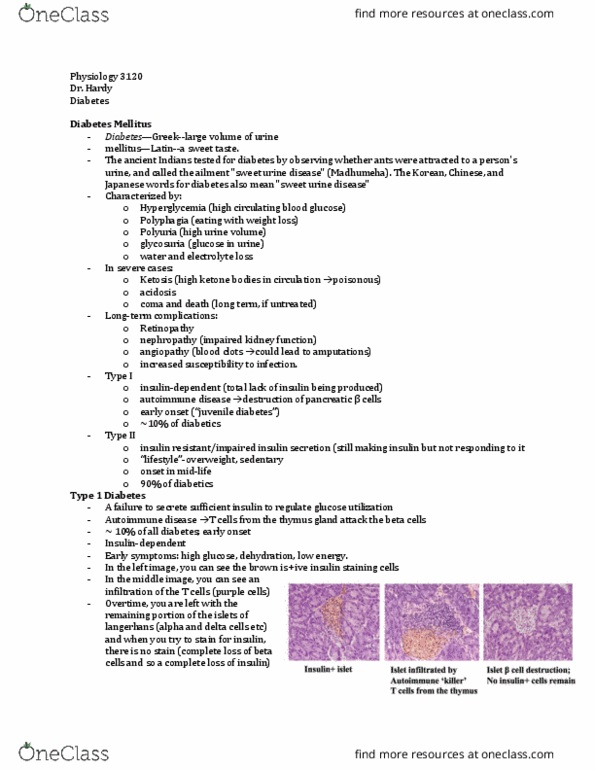
- Images: NOD mouse (non-obese diabetec)
o Over time, the mouse develops type 1 diabetes
o Before full progression of type 1 diabetes, there are insulin positive beta cells
o As the disease progresses, there are implications of the T cells (normally they are helping
you, but here they attack the beta cells and destroy them)
o Over time you are left with the remaining portion of the islets of Langerhans (alpha cells,
delta cells)
▪ If you try to stain for insulin, there are no beta cells remaining
o COMPLETE LOSS OF BETA CELLS = LOSS OF INSULIN PRODUCTION
find more resources at oneclass.com
find more resources at oneclass.com

What happens without Insulin?
- High levels of glucose circulating in the body is a big deal
- Inability to transport glucose into cells --alternate energy source ne eded!
o Protein, Fat
o Adipose and muscle can not bring glucose into those organs. These cell types need energy
▪ Lack insulin, therefore inability to bring glucose into organs via activation of GLUT4
- Both cell types need to find alterative ways to generate ATP
o They do short term, but long term this is detrimental
o Break down fat and protein to generate and liberate more ATP (used to make glucose in
other organs)
Other sources of Energy-Protein
- Increase gluconeogenesis
- Muscle broken down to AA
o If you are a muscle cell, you should break down muscle to amino acids
o Animal that does not have insulin, there is overall muscle wasting. The muscle is degraded
(breaks down and increases amino acids)
- AA converted to glucose in liver (used by liver, brain)
o The amino acids that are liberated from breaking down muscle and protein can be sued to
make glucose, inside the muscle AND inside the liver to generate more glucose and ATP for
the livers needs
o Muscle is taking a hit to help the liver, to generate energy
- Results in:
o Muscle wasting
o Weight loss
▪ Type 1 diabetics lose weight because they are losing muscle waste
find more resources at oneclass.com
find more resources at oneclass.com