Pathology 2420A Lecture Notes - Lecture 11: Inflammatory Bowel Disease, Ulcerative Colitis, Regulatory T Cell

17 Dec 2016
School
Department
Course
Professor

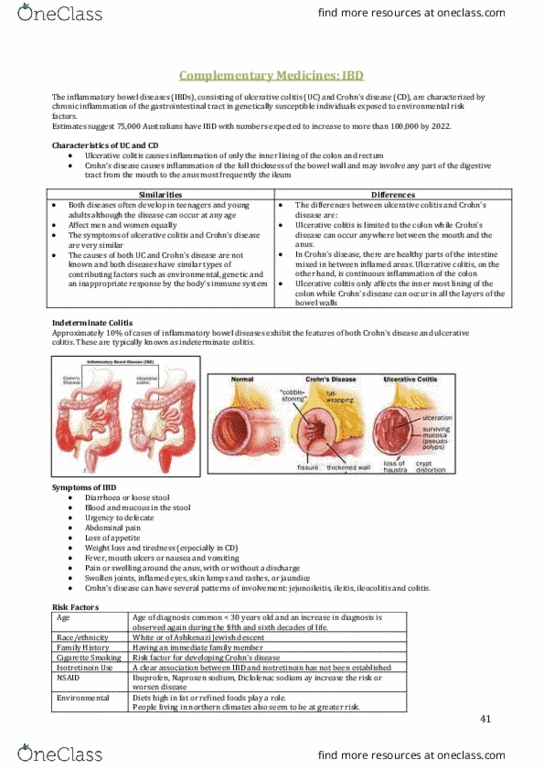
Inflammatory Bowel Disease
IBD includes 2 diseases of unknown etiology:
- Ulcerative Colitis (UC)
- Crohn’s Disease (CD)
These are both inflammatory diseases, with a peak age of onset between ages
15 and 35.
- Chronic diarrhea
- Lifelong exacerbations and remissions
- Extraintestinal problems involving liver, joints, skin, and the eye
IBD: unregulated and exaggerated local immune responses to gut microbes in
genetically susceptible individuals. About 15% of IBD patients have an affected
first degree relative. 50% in monozygotic twins with CD. Although the gut flora is
important, no specific microbe has been identified. The microbes might be
triggering the abnormal immune response. The exaggerated immune response is
due to too much T-cell activation and/or too little control by regulatory T cells.
While Crohn’s disease typically involves the small and large intestine in a
segmental manner with intervening skip areas, ulcerative colitis is generally a
disease a continuity that starts in the rectum and progresses in a retrograde
fashion to involve varying lengths of the colon.
Crohn’s Disease: Any part of the gut from the mouth to anus may be involved,
but most commonly the small bowel (especially the far end, called the terminal
ileum) and/or large bowel are affected. Segments of involved bowel are
separated by normal bowel (segmental involvement with skip lesions). This
disease affects all layers of the bowel wall and produces chronic inflammation
and scarring (transmural chronic inflammation and fibrosis). Granulomas are
frequently present. The early lesions are tiny ulcers. With progression, the ulcers
enlarge and become long, serpentine, and fissuring (go deep into bowel wall).
The bowel wall thickens and there is narrowing of the lumen (stenosis). With
time, the fissures may lengthen to form sinuses leading to abscesses or fistulas
to other bowel loops or other organs.
Patients have episodes of diarrhea, pain and fever. There may be overt or occult
blood in the stools, but massive bleeding is uncommon. Medical treatment
involves anti-inflammatory agents. CD cannot be cured by surgery. Surgery is
therefore limited to resection of complications (fistulas, stenosis) and over a
lifetime several operations may be necessary.
Ulcerative Colitis: Involves only large bowel, most commonly the rectum and
left colon, but may also involve the entire large bowel. This disease affect only
the lining of the large bowel, and is not transmural like CD. The rectum is always
involved, and the area affected extends proximally in a continuous manner with
no skip areas. Microscopically, the bowel lining shows acute and chronic
inflammation and ulcers. Granulomas are not seen. During exacerbations, the
mucosal lining is red, swollen, and bleeding with small to large shallow ulcers.
Because it is not transmural, strictures, abscesses, and fistulas do not occur.
Typically, patients have chronic bloody diarrhea and pain. Severity ranges from
mild to severe, and may sometimes be fatal. Patients with longstanding
ulcerative colitis are at increased risk of developing large bowel cancer.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
These are both inflammatory diseases, with a peak age of onset between ages. Extraintestinal problems involving liver, joints, skin, and the eye. Ibd: unregulated and exaggerated local immune responses to gut microbes in genetically susceptible individuals. About 15% of ibd patients have an affected first degree relative. Although the gut flora is important, no specific microbe has been identified. The microbes might be triggering the abnormal immune response. The exaggerated immune response is due to too much t-cell activation and/or too little control by regulatory t cells. Crohn"s disease: any part of the gut from the mouth to anus may be involved, but most commonly the small bowel (especially the far end, called the terminal ileum) and/or large bowel are affected. Segments of involved bowel are separated by normal bowel (segmental involvement with skip lesions). This disease affects all layers of the bowel wall and produces chronic inflammation and scarring (transmural chronic inflammation and fibrosis).