HTHSCI 2F03 Lecture Notes - Lecture 13: Osteotomy, Paracetamol, Gracilis Muscle

26 Dec 2020
School
Department
Course
Professor
The Shoulder
Shoulder Dislocation
Classification
Anterior
95% of shoulder dislocations.
Direct trauma or falling on hand
Humeral head dislocates antero-inferiorly
Posterior
Caused by direct trauma or muscle contraction
(seen in epileptics).
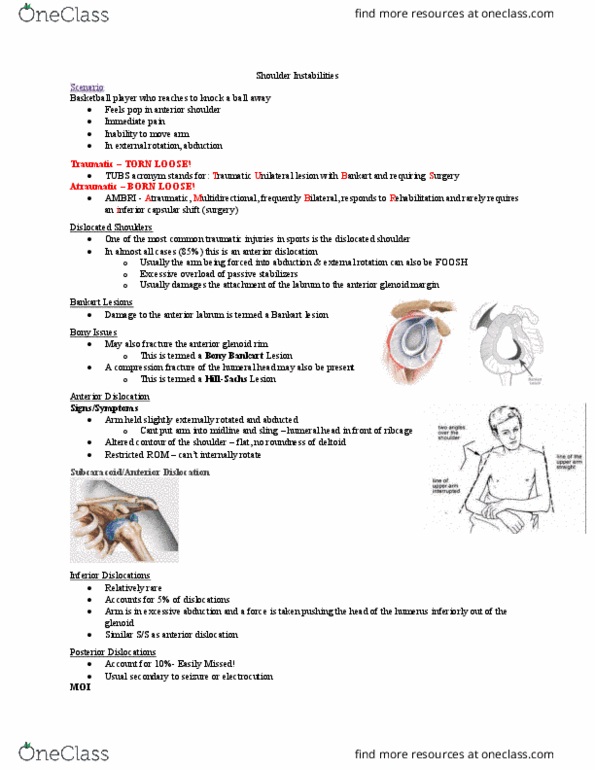
Associated Lesions
Bankart Lesion
Damage to anteroinferior glenoid labrum.
Hill-Sachs Lesion
Cortical depression in the posterolateral part of the
humeral head following impaction against the glenoid
rim during anterior dislocation.
Occurs in 35-40% of anterior dislocations.
Presentation
Shoulder contour lost: appears square
Bulge in infraclavicular fossa: humeral head
Arm supported in opposite hand
Severe pain
Specific Management
Assess for neurovascular deficit: esp. axillary N.
Sensation over “chevron” area before and after
reduction.
Occurs in 5%
X-ray: AP and transcapular view
Reduction under sedation (e.g. propafol)
Hippocratic: Longitudinal traction c
¯ arm in 30O
abduction and counter traction @ the axilla
Kocher’s: external rotation of adducted arm,
anterior movement, internal rotation
Rest arm in a sling for 3-4wks
Physio
Complications
Recurrent dislocation
90% of pts. <20yrs with traumatic dislocation
Axillary N. injury
Recurrent Shoulder Instability
TUBS: Traumatic Unilateral dislocations with a Bankart lesion
often require Surgery
Mostly young patients: 15-30yrs
Surgery involves a Bankart repair
AMBRI: Atraumatic Multidirectional Bilateral shoulder
dislocation is treated with Rehabilitation, but may require
Inferior capsular shift
Impingement Syndrome / Painful Arc
Pathology
Entrapment of supraspinatus tendon and subacromial
bursa between acromion and grater tuberosity of
humerus.
→ subacromial bursitis and/or supraspinatous
tendonitis
Presentation
Painful arc: 60-120O
Weakness and ↓ ROM
+ve Hawkin’s test
Ix
Plain radiographs: may see bony spurs
US
MRI arthrogram
Rx
Conservative
Rest
Physiotherapy
Medical
NSAIDs
Subacromial bursa steroid ± LA injection
Surgical
Arthroscopic acromioplasty
Differential of Painful Arc
Impingement
Supraspinatous tear or partial tear
AC joint OA
Frozen Shoulder: Adhesive Capsulitis
Presentation
Progressive ↓ active and passive ROM
↓ ext. rotation <30O
↓ abduction <90O
Shoulder pain, esp. @ night (can’t lie on affected side)
Cause
Unknown, may follow trauma in elderly
Commonly assoc. c
¯ DM
Rx
Conservative: rest, physio
Medical
NSAIDs
Subacromial bursa steroid ± LA injection
Rotator Cuff Tear
2
O to degeneration or a sudden jolt or fall
Partial tears → painful arc
Complete tear
Shoulder tip pain
Full range of passive movement
Inability to abduct the arm
Active abduction possible following passive
abduction to 90O
Lowering the arm beneath this → sudden drop
“drop arm” sign
Rx: open or arthroscopic repair
© Alasdair Scott, 2012
116
Supracondylar Fractures of the Humerus
Presentation
Common in children after FOOSH
Elbow very swollen and held semi-flexed.
Sharp edge of proximal humerus may injure brachial
artery which lies anterior to it.
Classification
Extension
Commonest type
Distal fragment displaces posteriorly
Gartland further classified extension type:
Type 1: non-displaced
Type 2: angulated c
¯ intact posterior cortex
Type 3: displaced c
¯ no cortical contact
Flexion
Less common
Distal fragment displaces anteriorly
Specific Management
Ensure there is no neurovascular damage
If radial pulse absent or damage to brachial
artery suspected, take urgently to theatre for
reduction ± on-table angiogram.
Median nerve is also vulnerable
Restore the anatomy
No displacement → flex the arm as fully as
possible and apply a collar and cuff for 3wks –
triceps acts as sling to stabilise fragments.
Displacement → MUA + fixation with K-wires +
collar and cuff with arm flexed for 3wks.
Specific Complications
Neurovascular Injury
Brachial artery
Radial nerve
Median nerve: esp. anterior interosseous branch
Supplies deep forearm flexors (FPL, lateral half
of FDP and pronator quadratus)
Compartment syndrome
Monitor closely during the first 24h
Pain on passive extension of the fingers (stretches
flexor compartment) is early sign.
Mx: try extension of the elbow, surgical Rx may be
needed.
Volkmann’s ischaemic contracture can result → fibrosis
of flexors → claw hand.
Gunstock Deformity
Valgus, varus and rotational deformities in the coronal
plane do not remodel and → cubitus varus.
Cubitus varus deformity is referred to as a “gunstock”
deformity.
© Alasdair Scott, 2012
117
Femoral and Tibial Fractures
Specific Management
Resus and Mx life-threatening injuries first.
X-Match
Tibial #: 2 units
Femoral #: 4 units
Assess neurovascular status: esp. distal pulses
If open
Abx and ATT
Take to theatre urgently for debridement,
washout and stabilisation
Fixation methods
Intramedullary nail
Ex-fix
Plates and screws
MUA c
¯ fixed traction for 3-4mo
Specific Complications
Hypovolaemic shock
Neurovascular
SFA: swelling and check pulses
Sciatic nerve
Compartment syndrome
Respiratory complications
Fat embolism
ARDS
Pneumonia
Ankle Injuries
Ligament Strains
Typically twisting inversion injury
Strains anterior talofibular part of lateral collateral
ligament
Medial deltoid ligament strains are rare.
May be assoc. c
¯ malleolar avulsion #s
Ankle Fracture
Ottowa Ankle Rules
X-ray ankle if pain in malleolar zone + in any of:
Tenderness along distal 6cm of posterior tib / fib
including posterior tip of the malleoli.
Inability to bear weight both immediately and in
ED
Weber Classification
Relation of fibula # to joint line
A: below joint line
B: at joint line
C: above joint line
Weber’s B and C represent possible injury to the
syndesmotic ligaments between tib and fib → instability
Mx
Weber A
Boot or below-knee POP
Non-displaced Weber B/C
Below-knee POP
Displaced Weber B/C
Closed reduction and POP if anatomical
reduction achieved
ORIF if closed reduction fails
© Alasdair Scott, 2012
118
Document Summary
Caused by direct trauma or muscle contraction (seen in epileptics). Cortical depression in the posterolateral part of the humeral head following impaction against the glenoid rim during anterior dislocation. Assess for neurovascular deficit: esp. axillary n. Sensation over chevron area before and after reduction. Hippocratic: longitudinal traction c arm in 30o abduction and counter traction @ the axilla. Kocher"s: external rotation of adducted arm, anterior movement, internal rotation. Rest arm in a sling for 3-4wks. Tubs: traumatic unilateral dislocations with a bankart lesion often require surgery. Ambri: atraumatic multidirectional bilateral shoulder dislocation is treated with rehabilitation, but may require. Entrapment of supraspinatus tendon and subacromial bursa between acromion and grater tuberosity of humerus. 2o to degeneration or a sudden jolt or fall. Inability to abduct the arm abduction to 90o. Lowering the arm beneath this sudden drop. Supplies deep forearm flexors (fpl, lateral half of fdp and pronator quadratus)