PSYC 444 Lecture Notes - Lecture 12: World Health Organization, Sleep Disorder, Circadian Rhythm

14 May 2018
School
Department
Course
Professor

PSYC 444 – LECTURE 12
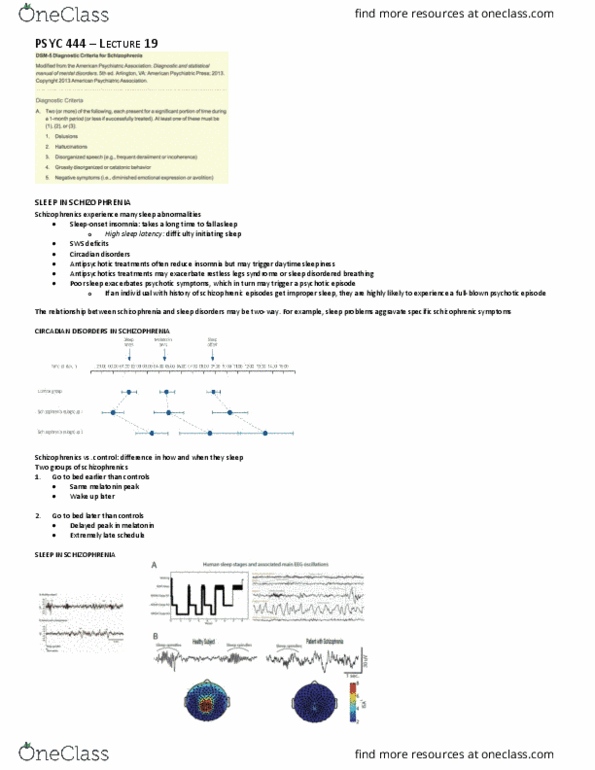
Information from WHO (World Health Organization)
(left): Higher quality of life (long life without disease) in green
(right): countries that should be doing well, given higher quality of life, are doing the worst in terms of sleep.
• North America and Europe are not sleeping well
o Sleep is not a priority in developed countries
• People are not feeling great, missing work, etc.
Insomnia is very costly, despite being something that is treatable.
INSOMNIA
Insomnia: difficulty initiating or maintaining sleep, in conditions where one should be able to sleep
• Most common sleep disorder
• Among the most prevalent of all mental health disorders
Insomnia severity is typically measured by the Insomnia Severity Scale (ISI)
INSOMNIA: DIAGNOSIS I OF III
Predominant complaint of dissatisfaction with sleep quality or quantity, associated with one or more of the following symptoms:
• Difficulty initiating sleep
• Difficulty maintaining sleep (characterized by frequent awakenings or problems returning to sleep after awakening)
• Early-morning awakening with inability to return to sleep
Note: it is not considered insomnia if you are able to fall back asleep after waking up; this would be fragmented sleep, another disorder
INSOMNIA: DIAGNOSIS II OF III
• The sleep difficulty occurs at least 3 nights per week, present for at least 3 months
• Sleep disturbance causes clinically significant distress or impairment in social, occupational, educational, academic, behavioral or other important areas of
functioning
Note: it is common to experience life occurrences that put you in a state of high excitement or nervousness, which, in turn, leads to difficulty sleeping. This is normal
and happens to all of us. Thus, the sleep difficulty must be chronic in order to be diagnosed as insomnia.
Note: Insomnia must cause psychological or physiological distress. If ou feel fie, it is ot isoia. Just eause ou ae uale to sleep the eoeded eight
hours, you are not an insomniac. For example, some people sleep five hours and feel fine; they are just short sleepers.
INSOMNIA: DIAGNOSIS III OF III
• The sleep difficulty occurs despite adequate opportunity for sleep.
• Insomnia is not better explained by and does not occur exclusively during course of another sleep-wake disorder (e.g. narcolepsy, breathing-related sleep
disorder, circadian rhythm sleep-wake disorder, parasomnia)
• Insomnia is not attributable to the physiological effects of a substance (e.g. drug of abuse, medication)
• Co-existing mental disorders and medical conditions do not adequately explain the predominant complaint of insomnia
Note: new mothers are frequently woken up by their child. Thus, their environment is preventing them from getting adequate opportunity for sleep.
Note: Caffeinated drinks (e.g. Red Bull) and drug of abuse (e.g. amphetamines) are commonly associated with inability to sleep
find more resources at oneclass.com
find more resources at oneclass.com

INSOMNIA PREVALENCE
The prevalence of chronic, clinically significant insomnia is about 10%
Advancing age, gender (female), and low SES are strong insomnia correlates
• NOT causing insomnia! Just correlated with insomnia
Prevalence depends on how you define insomnia
• Sleep clinics are still rare and prevalence is not tracked well
• Different definitions of insomnia used across different clinics
INSOMNIA HEALTH RISKS
Insomnia is, itself, a risk factor for a wide variety of psychological, psychiatric, and medical disorders, including depression, substance abuse, and hypertension
INSOMNIA AND MENTAL HEALTH: CHICKEN AND EGG PROBLEM
Although isoia is oelated ith a etal health issues, e do’t ko hethe it is the etal health issues that lead to insomnia or insomnia that leads to
depression, for example.
However, more research is showing that trouble sleeping either exacerbates current mental health problems or acts as a trigger. Thus, insomnia itself seems to be the
fial push toads deelopetal of a etal disode. Fo eaple, diffiult sleepig a tigge a pshoti episode.
INSOMNIA AND DEPRESSION
There is now strong evidence supporting the relationship between insomnia and subsequent development of depression
• A large body of research established that insomnia is a significant risk factor for depression, as seen in a recent meta-analysis.
• Insomnia resulted in nearly 2x greater risk for developing depression
• Increased odds ratio: OR = 1.10-3.51
INSOMNIA AND SUICIDE
There is considerable evidence that insomnia is a risk factor for suicide.
• In a recent meta-analysis, insomnia symptoms were significantly associated with suicidal ideation, attempt or completion (OR = 1.63-2.41) after adjusting
for comorbidities.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Information from who (world health organization) (left): higher quality of life (long life without disease) in green (right): countries that should be doing well, given higher quality of life, are doing the worst in terms of sleep. North america and europe are not sleeping well. Sleep is not a priority in developed countries. People are not feeling great, missing work, etc. Insomnia is very costly, despite being something that is treatable. Insomnia: difficulty initiating or maintaining sleep, in conditions where one should be able to sleep: most common sleep disorder. Among the most prevalent of all mental health disorders. Insomnia severity is typically measured by the insomnia severity scale (isi) Predominant complaint of dissatisfaction with sleep quality or quantity, associated with one or more of the following symptoms: Difficulty maintaining sleep (characterized by frequent awakenings or problems returning to sleep after awakening) Early-morning awakening with inability to return to sleep.