PHGY 209 Lecture Notes - Lecture 10: Thromboxane A2, Phospholipid, Aspirin

5 Oct 2017
School
Department
Course
Professor
Document Summary
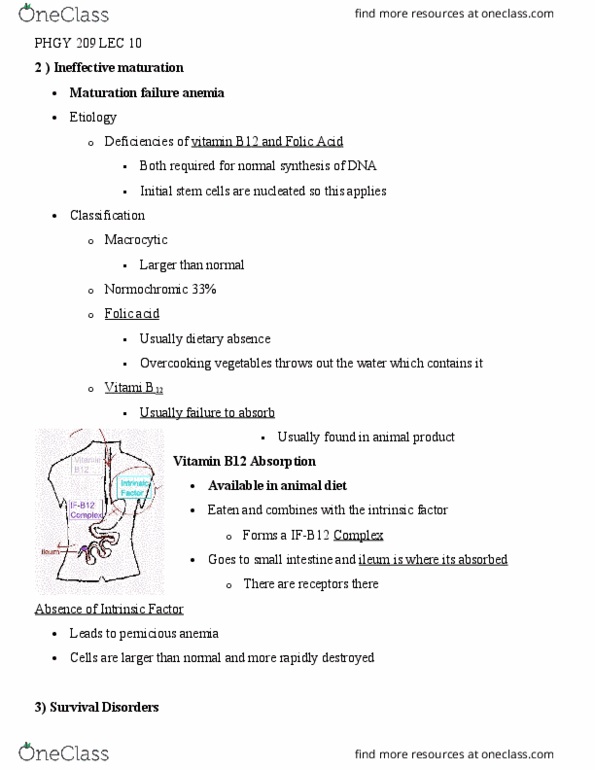
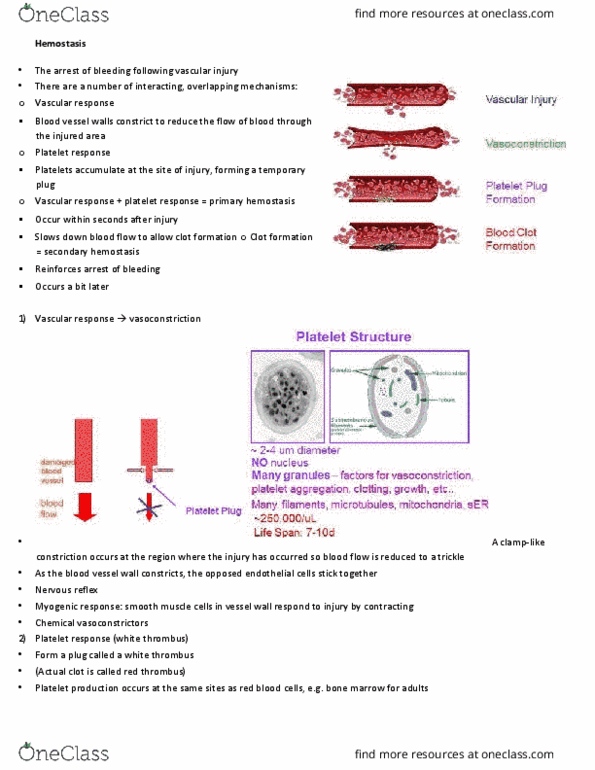
Hemolytic anemias may be accompanied by jaundice. Etiology: congenital, acquired, abnormal membrane structure (less flexible, more fragile, abnormal enzyme systems (abnormal metabolism, abnormal hb structure (sickle cell anemia), thalassemia deficient synthesis of globin amino acid chains) A number of interacting overlapping mechanisms: primary and secondary hemostasis: vascular response. The opposed endothelial cells stick together: nervous reflex, myogenic response smooth muscle cells in vessel wall respond to injury by contracting, chemical vasoconstrictors, platelet response. A platelet plug comes in to stop the bleeding: structure of platelets: Many granules factors for vasoconstriction, platelet aggregation, clotting, growth, etc. Platelet production***: needs thrombopoietin (mostly from liver, pluripotential stem cell turns into committed stem cell, then megakaryocytes and finally platelets. Prostacyclin (no) allows movement in the blood vessel. Collagen facilitates the binding of proteins together. Platelets release thromboxane a2 which acts as a vasoconstrictor. Platelets produce atp and serotonin, release plate factors: adhesion, activation and release of cytokines which increase the aggregation, aggregation, consolidation.