NUR1 319 Lecture Notes - Lecture 6: Atypical Antipsychotic, Metformin, Electrocardiography

11 May 2016
School
Department
Course
Professor
Document Summary
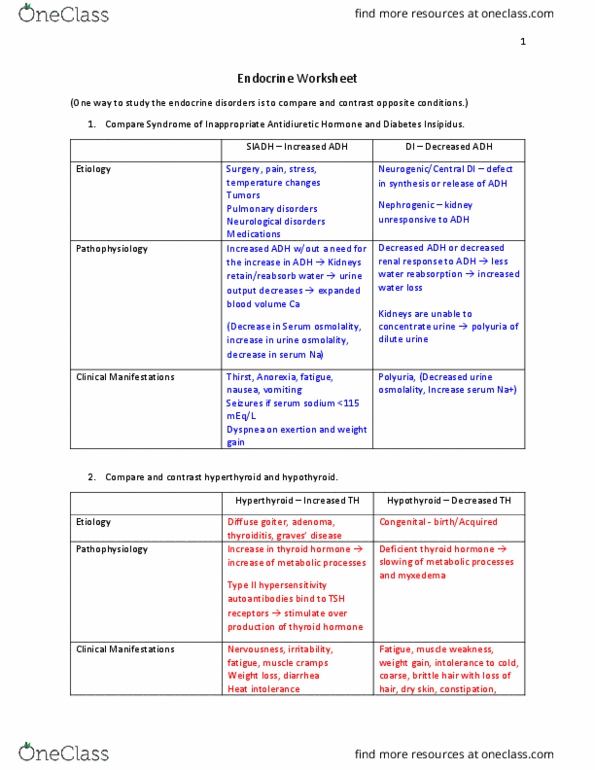
Inability to produce adh, antidiuretic hormone or vasopressin who promote reabsorption of water at the kidneys prevent dehydration, stimulate high blood osmolality (sensed in hypothalamus) Nature of dysregulation: ecf deficit (dehydration), insufficient intake of and electrolytes, excessive fluid loss through secretions or excretions. Causes: inadequate synthesis of adh, injury, cancer, leukemia, kidney water disease. Sign symptoms: acute weight loss second to polyuria and. Polidipsia, decreased skin turgor, dry mucous, dry tongue, change behavior (agitation, restlessness, and weakness), flat neck vein, weak pulses, slow filling peripheral veins and orthostatic hypotension. Pt with no di: quickly result in decrease urine output. Pt with di: will continue to output urine. Di treatment: fluid resuscitation (isotonic fluid) and e+ replacement. Admin iv: desmopressin (ddavp) to decrease urine output, tegretol (increase kidney response to adh), thiazide diuretic (decrease na+ reabsorption) and chlorpropamine (adh effect) Monitor vital and neuro signs (assess neuro status) Assess urine for amount, color and specific gravity.