MEDI7111 Lecture Notes - Lecture 10: Thiazide, Magnesium, Pituitary Adenoma


Endocrine 10
Hyperparathyroidism
Aetiology
Hyperparathyroidism is categorised into primary, secondary and tertiary with regard to
aetiology.
Primary Hyperparathyroidism
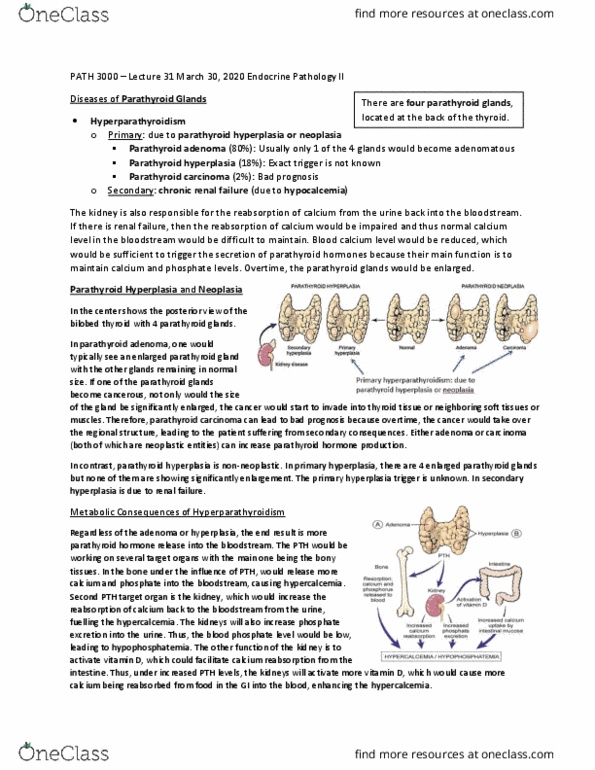
Primary HPT is due to a pathology originating in the parathyroid gland, resulting in autonomous
production of PTH which is not responsive to normal negative feedback mechanisms. The most
common pathology is a single adenoma (80% of cases), followed by hyperplastic glands (15%),
multiple adenomas (3%) and rarely carcinoma (1%).
Parathyroid Hyperplasia Parathyroid Adenoma
Secondary Hyperparathyroidism
Secondary HPT is pathological compensation for hypocalcaemia caused by pathology in another
organ. This is often due to renal failure or malignancy (e.g. small cell lung cancer secreting
PTHrP).
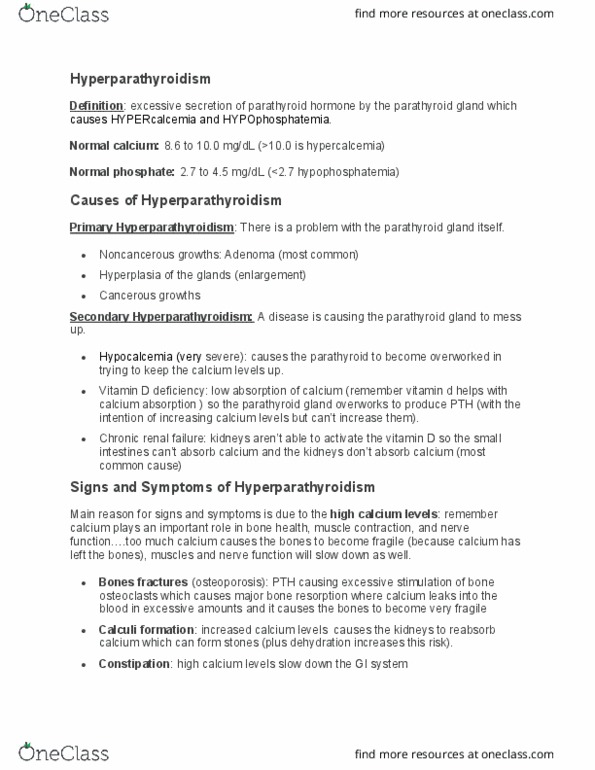
Chronic renal failure stimulates PTH secretion in a number of ways:
Low GFR
o phosphate excretion ↓
Serum phosphate has a stimulatory effect on PTH and suppressed
vitamin D synthesis (patients with CKD should be on a low phosphate
diet to help mitigate this effect)
hydroxylation of 25(OH) Vitamin D 1,25(OH) Vitamin D ↓
oImpaired calcium absorption from the gut
o negative feedback to PTH production ↓
Tertiary Hyperparathyroidism
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Hyperparathyroidism is categorised into primary, secondary and tertiary with regard to aetiology. Primary hpt is due to a pathology originating in the parathyroid gland, resulting in autonomous production of pth which is not responsive to normal negative feedback mechanisms. The most common pathology is a single adenoma (80% of cases), followed by hyperplastic glands (15%), multiple adenomas (3%) and rarely carcinoma (1%). Secondary hpt is pathological compensation for hypocalcaemia caused by pathology in another organ. This is often due to renal failure or malignancy (e. g. small cell lung cancer secreting. Chronic renal failure stimulates pth secretion in a number of ways: Tertiary hpt follows secondary hpt, as the underlying pathology causing the calcium derangement has resolved (e. g. renal transplant, remission of cancer), but the parathyroid gland is continuing to secrete excess pth. This is often due to hyperplasia/adenoma of the parathyroid glands in response to the prolonged hypocalcaemia.