IMM2022 Lecture Notes - Lecture 3: Serum Sickness, Antigen Presentation, Macrophage

30 May 2018
School
Department
Course
Professor

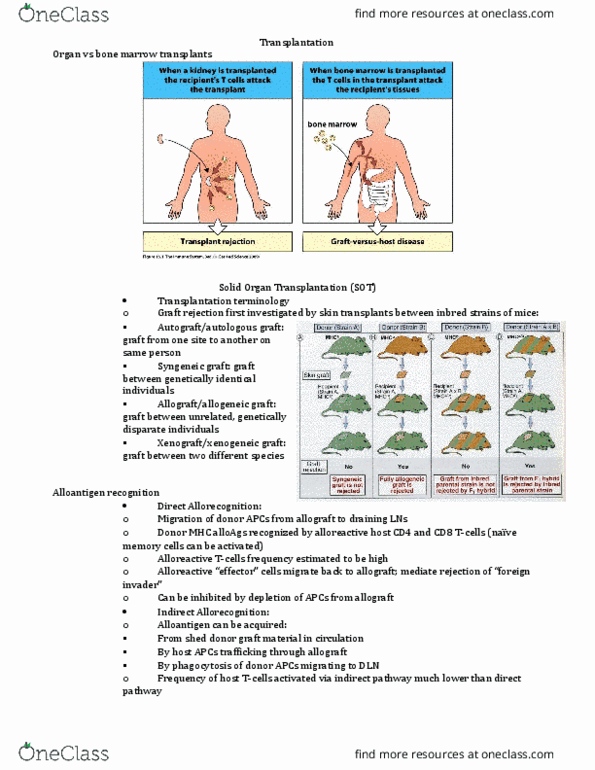
TRANSPLANTATION
Skin grafts
Autograft
o Same individual
Isograft
o Genetically identical individuals
Solid organ transplant
Allograft
o Between different members
of the same species
o Genetically non-identical
Xenograft
o Transfer of xenogeneic tissue
o Different species
• Pre transplant assessment: compatibility
o ABO blood group matching:
-Preformed anti-blood group antibodies: IgM -> hyperacute rejection
-Pre-transplant reduction of antibody (eg. Plasma exchange, neutralise antibody, decrease
antibody production via splenectomy or rituximab)
o Human leukocyte antigen (HLA) matching:
-Stimulates strong rejection responses are encoded by MHC genes
-Human MHC = HLA
-HLA class I genes; HLA-A, -B, and –C
-HLA class II genes; HLA-DR, -DQ, and –DP
find more resources at oneclass.com
find more resources at oneclass.com

-has extensive polymorphism exhibited
-matching HLA improves graft survival
o Risk of graft rejection (pre-existing antibodies):
-Clinical history which may suggest pre-sensitisation (eg. Previous blood transfusion,
transplant, pregnancy -> exposed to partner)
-assess reactivity to a panel of donor antigens
-inherited?
o Pre-transplant cross-matching:
-cytotoxic PRA testing (high PRA testing = longer waiting times, increased rejection episodes,
greater immunosuppression, decreased graft survival)
-can identify specific antigens to avoid for a particular recipient
o Pre-transplant testing:
HLA typing -> high resolution matching for bone marrow or hematopoietic stem cell
transplantation (condition the patient, get rid of all B and T cells) -> logistically impossible to
match for most solid organ transplants (happens very quickly , take whatever you can get)
• Rejection:
o Skin graft rejection is the result of T cell mediated anti-graft response
Hyperacute graft
rejection
o Graft failure in minutes – hours after transplant
o Due to pre-sensitisation of recipient to graft antigens (ABO and
HLA) by prior blood transfusions, transplants, pregnancy
o Preformed antibodies, B cell mediated, ABO blood groups, HLA
molecules
Acute graft rejection
o Initial healing and vascularisation
o Mononuclear cells infiltrate graft (lymphocytes and
macrophages)
o 1-2 weeks later vascular changes
o Is reversible
o Tissue necrosis
o Endothelial cell proliferation
o Need to increase immunosuppression
o T cell mediated, HLA molecules
Chronic graft rejection
o Graft failure in months-years
o The worst rejection
o Progressive narrowing of the arteries due to excessive fibrosis
and smooth muscle cell proliferation around vessels
o Cause unknown
o Generall not reversible (don’t get enough ogen, no blood
flow)
• Graft vs host disease
(GvHD):
o T cell mediated against host
o Skin rash, liver dysfunction, inflammation of gut,
nausea/vomiting
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Allograft: between different members of the same species, genetically non-identical. Xenograft: transfer of xenogeneic tissue, different species, pre transplant assessment: compatibility, abo blood group matching: Preformed anti-blood group antibodies: igm -> hyperacute rejection. Pre-transplant reduction of antibody (eg. plasma exchange, neutralise antibody, decrease antibody production via splenectomy or rituximab: human leukocyte antigen (hla) matching: Stimulates strong rejection responses are encoded by mhc genes. Hla class i genes; hla-a, -b, and c. Hla class ii genes; hla-dr, -dq, and dp. Matching hla improves graft survival: risk of graft rejection (pre-existing antibodies): Clinical history which may suggest pre-sensitisation (eg. previous blood transfusion, transplant, pregnancy -> exposed to partner) Assess reactivity to a panel of donor antigens. Cytotoxic pra testing (high pra testing = longer waiting times, increased rejection episodes, greater immunosuppression, decreased graft survival) Can identify specific antigens to avoid for a particular recipient: pre-transplant testing: