BMS2031 Lecture Notes - Lecture 23: Blood Gas Tension, Collecting Duct System, Cardiac Output

31 May 2018
School
Department
Course
Professor

Week 9. Respiratory 4, 5&6 Transport of gases,
Control of respiration and, Regulation of acid base
balance
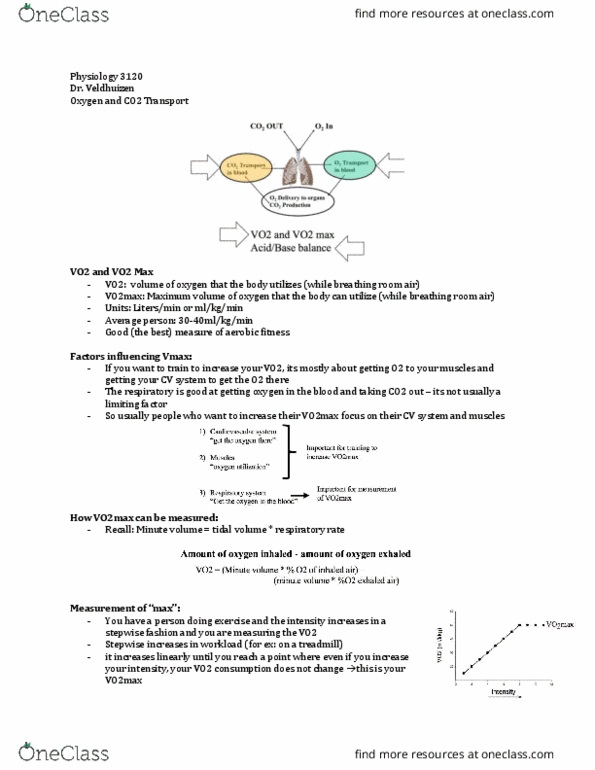
TRANSPORT OF GASES
• Humans at rest need 250ml of oxygen per minute to support cellular activities in the tissues
• Solubility of O2 in blood is 2ml/L
• A sedentary person has a VO2 Max of around 20ml of O2 per kg of body weight per minute of
exercise
• A highly trained endurance athlete can have a VO2 Max of around 70ml/kg/min
• Oxygen consumption:
o Pressure gradient drives diffusion of O2 from alveolus to blood and from blood to tissues
o Diffusion continues until equilibrium is reached
o Normally there is sufficient time for equilibrium to be reached in the alveolus before the
blood reaches the end of capillaries
• Oxygen transport:
o At atmospheric pressure, each litre of blood contains equivalent 200ml of O2
Transported in 2 ways
1. Dissolved in plasma and erythrocyte cytoplasm (depends on PP outside)
-Her’s la predits that the aout dissoled ill e proportioal to PO2 hih is
around 3ml/100ml plasma
2. Reversibly bound to haemoglobin (Hb) – roughly 197ml of O2
o When percent of O2 saturation of haemoglobin <60% this becomes an issue for
breathing
• Measuring O2 saturation:
o Finger pulse oximeter
o PO2 < 60mmHg (hypoxia) is considered lowest acceptable PO2 in an ICU patient – means
you start driving respiration through O2 and not CO2
• Lungs can become quite diseased before you see a significant effect of O2 unloading on tissues
find more resources at oneclass.com
find more resources at oneclass.com

• Factors affecting O2/Hb dissociation:
o Bohr effect – shifts ure to the right (tissues get ore O2 eause it does’t sta oud
to Hb strongly – offloads more)
o Decrease pH
o Increased PCO2
o Increased 2,3 – DPG
o eg. during exercise: faster metabolism, pH decreases, produce more CO2/lactic acid,
temperature goes up and RBC producing more DPG
• factors affecting arterial oxygen:
• CO2 transport:
Is transported in 3 forms
1. CO2 = 10% - dissolved in plasma and cytoplasm of RBC
2. Hgb.CO2 = 30% - when no O2
3. HCO3- = 60% - majority (maintains balance by Cl-)
• Eg. Anne is a competitive cyclist and showed resting O2 consumption of 200ml/min with resting
cardiac output of 5L/min
o She has increased CO (5 to 25L)
o Increased perfusion of lungs
o Increased ventilation
o Hb-O2 saturation curve moves to the right (decreased pH, increased temperature,
increased DPG -> offloading more O2)
o Diffusion of O2 ~0.25 (normally 0.75) sec during exercise which is still enough time for
equilibration (enough time to completely saturate Hb)
o Also still enough time to unload CO2 (not really an issue – more soluble than O2)
find more resources at oneclass.com
find more resources at oneclass.com

o In exercise, up to 80% O2 is unloaded from Hb – steepness of the curve is at 40-15mmHg
• CO poisoning:
o Hb has a much higher affinity for CO than O2 – 250 times greater
o Hb binding site for both is the same
o CO competes equally for Hb
- at alveolar pressure of 0.4mmHg – half of Hb will bind with CO instead
-at alveolar pressure 0.6mmHg (LETHAL) – more CO will bind to Hb than O2
o CO bound to Hb reduces that ability of any bound O2 to unload
-> body thinks everythig’s oka
o Not very specific symptoms:
Headaches
Nausea
Drowsiness
o PO2 is normal so the body does not detect hypoxia
o Treatment = ventilation with O2 or hyperbaric O2
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Control of respiration and, regulation of acid base balance. Transported in 2 ways: dissolved in plasma and erythrocyte cytoplasm (depends on pp outside) Increased 2,3 dpg: eg. during exercise: faster metabolism, ph decreases, produce more co2/lactic acid, temperature goes up and rbc producing more dpg factors affecting arterial oxygen, co2 transport: Is transported in 3 forms: co2 = 10% - dissolved in plasma and cytoplasm of rbc, hgb. co2 = 30% - when no o2, hco3- = 60% - majority (maintains balance by cl-, eg. Anne is a competitive cyclist and showed resting o2 consumption of 200ml/min with resting cardiac output of 5l/min: she has increased co (5 to 25l) At alveolar pressure of 0. 4mmhg half of hb will bind with co instead. At alveolar pressure 0. 6mmhg (lethal) more co will bind to hb than o2: co bound to hb reduces that ability of any bound o2 to unload. > body thinks everythi(cid:374)g"s oka(cid:455: not very specific symptoms: