BCMB30011 Lecture Notes - Lecture 32: Anterior Cruciate Ligament Injury, Branched-Chain Amino Acid, Body Composition

11 Aug 2018
School
Department
Course
Professor

Lecture 32
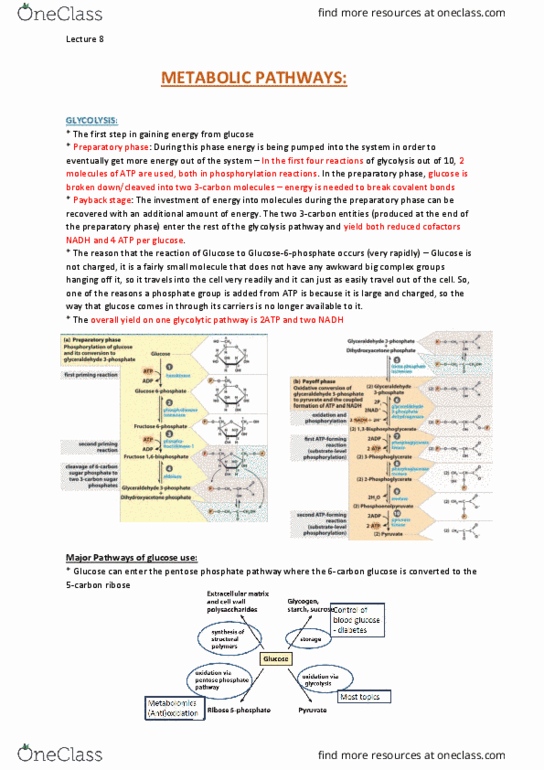
DISEASES & METABOLIC PATHWAYS:
Adipocyte metabolism in Type 1 diabetes or when the insulin receptor is blocked:
* Type 1 diabetes – situation where individual is lacking in
insulin
* Adipocytes have the GLUT 4 receptor just like myocytes.
* Primary defect is that the beta cells are destroyed so there is
no insulin released so the insulin receptor can’t be activated
and therefore the migration of GLUT 4 is blocked and
therefore there is no glucose uptake and therefore there is
less substrate for synthesis generally, so there’s less energy
provision through glycolysis and oxidation of pyruvate and
there’s also less of the pentose phosphate pathways.
* The lipid droplets have protein around the outside (perilipins)
which under the condition of mobilisation phosphorylation
occurs and allowing lipolysis to take place so therefore there
is mobilisation of fatty acids as an alternative source of
energy, and there’s also the formation of ketone occurring to
some extent.
* Similar changes occur in muscle, except myocytes do not
store TAG and release fatty acids by lipolysis. Myocytes take
up the fatty acids released from adipocytes
Dyslipidaemia and insulin resistance:
* In a situation where there is insulin resistance, a hormone sensitive lipase (HSL) which is
responsible for mobilising fatty acids from TAG in adipose tissue is upregulated so that there is more
release of free fatty acids (FFA) into the blood stream. The activity of lipoprotein lipase decreases
and this means that you’re not putting/storing lipids from VLDL & chylomicrons into adipocytes. The
fatty acids enter the liver, they get converted to the TAG which are incorporated into VLDL. Dietary
fat coming in from food cause increases in chylomicron delivery of TAG and because of the decrease
in lipoprotein lipase, there is more delivery of TAG from the diet to the liver because it’s not being
used by muscle or stored in adipose tissue on the way from the intestines to the liver. So, overall
there are higher levels of VLDL which are metabolically a bit different from the normal VLDL because
they are bigger than the normal VLDL and this also impacts the conformation of the proteins that are
associated on the outside of the VLDL. Also, with eating, apart from fat absorption is that there is
also glucose taken up and in the situation where glucose is not being effectively taken up into
muscles particularly, but also adipose tissue then the metabolism of glucose contributes to denovo
lipid synthesis (DNL).
* When lipoprotein particles interact in the plasma, one of the important proteins in the cholesteryl
ester transfer protein and its activity when HDL & VLDL are around, it donates cholesteryl ester from
HDL in exchange for TAG from either VLDL or LDL. The exchanges taking place are driven by the
increased level of TAG in the plasma because increased VLDL means increased TAG and increased
ApoB 100 in plasma as well. So, as a result of those changes, LDL becomes TAG rich, it can exchange
its cholesteryl ester with VLDL and therefore LDL is a substrate for hepatic lipase which produces the
small dense LDL which are more atherogenic because they can hang around more in blood vessels,
get through the endothelium, create the fatty streak and go on to develop atherosclerosis.

Lecture 32
*Similarly, HDL becomes relatively TAG rich, it’s still primarily responsible for carrying cholesteryl
ester, and as a result it’s also a good substrate for hepatic lipase and HDL after action by the hepatic
lipase becomes more vulnerable to degradation and ApoA1 can be lost through the kidney.
* So, overall there is a lower HDL, elevated VLDL and higher levels possibly of total LDL but certainly
higher levels of the dense LDL particle which is a health issue.
Insulin resistance and muscle protein:
In the absence of insulin there is no uptake of amino acids as readily by muscles, no synthesis of
proteins and no inhibition of protein breakdown. Instead, amino acids are released to the liver
(amino acids are released due to the degradation, particularly alanine and glutamine are the forms
in which the skeletons get to the liver) for gluconeogenesis/more glucose. This contributes further to
hyperglycaemia.
Case study: Muscle atrophy in injured soccer player:
* 24-year-old English Premier League soccer player
* Height 179 cm
* Body mass 78 kg
* Sustained a total rupture of the anterior cruciate ligament
(ACL) and injury to the external meniscus (part of the padding
between the bones) during a tackling motion
* Surgery 4 days after the injury occurred
* Study: Body composition scans by dual-energy X-ray
absorptiometry (DXA) to determine % fat mass and lean mass
in the affected leg at 4-weekly intervals. Compare immobilised leg to other leg.
Low carbohydrate (CHO)-high protein diet for the athlete was given in the study:
–<2.5 g/kg CHO
–2 to 2.5 g/kg protein (high protein as they thought it would be a good way to minimise losses)
–1 to 1.5 g/kg fat (quite low fat)
Document Summary
Adipocyte metabolism in type 1 diabetes or when the insulin receptor is blocked: * type 1 diabetes situation where individual is lacking in insulin. * adipocytes have the glut 4 receptor just like myocytes. * similar changes occur in muscle, except myocytes do not store tag and release fatty acids by lipolysis. Myocytes take up the fatty acids released from adipocytes. The activity of lipoprotein lipase decreases a(cid:374)d this (cid:373)ea(cid:374)s that you"re not putting/storing lipids from vldl & chylomicrons into adipocytes. The fatty acids enter the liver, they get converted to the tag which are incorporated into vldl. * when lipoprotein particles interact in the plasma, one of the important proteins in the cholesteryl ester transfer protein and its activity when hdl & vldl are around, it donates cholesteryl ester from. Hdl in exchange for tag from either vldl or ldl.