PHR 4111 Lecture Notes - Lecture 2: Hypotension, Procaine, Ventricular Tachycardia

8 Feb 2018
School
Department
Course
Professor
Document Summary
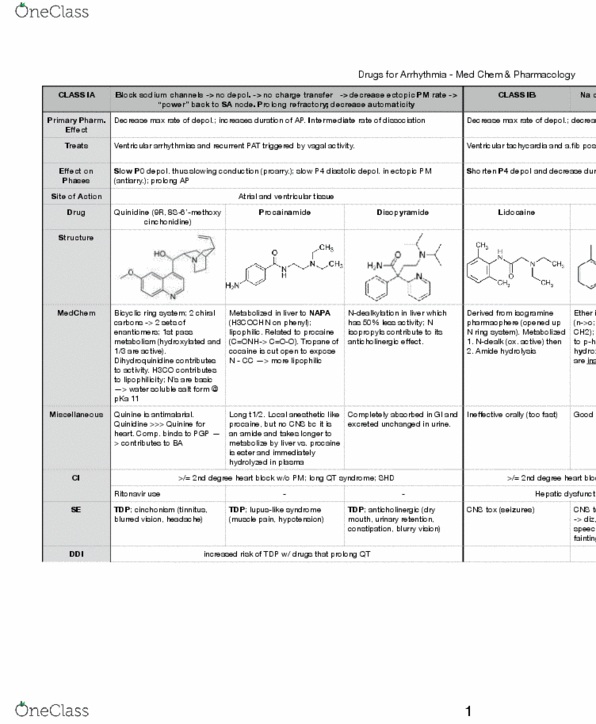
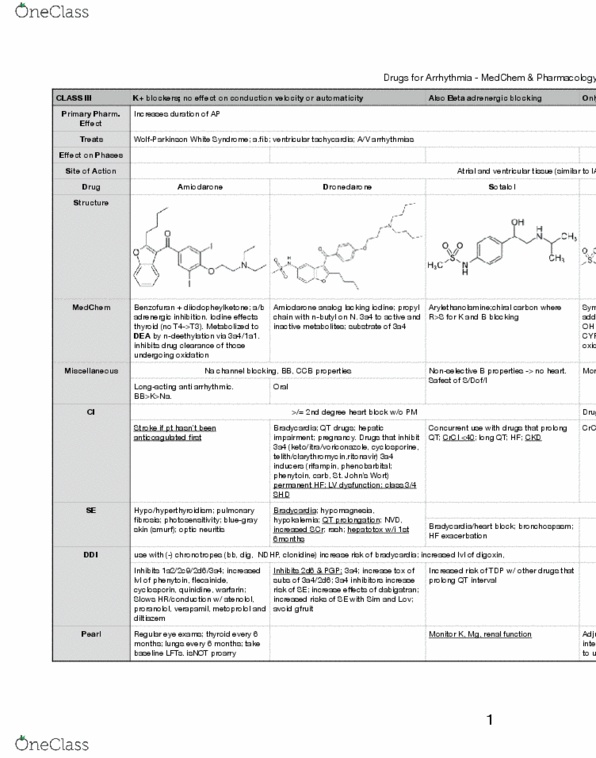
Na channel blockers (most potent) -> no depol. No e ect on refractory, decreased automaticity, slows conduction. Decreases max rate of depolarization; no change in duration of ap. Prevents pat and recurrent tachyarrhythmias associated with abnormal conduction and high mortality. 1st is less active and lactam metabolite is inactive and ng for arrhythmia. Structural analog of procainamide (aliphatic n is part of n-methyl piperidine ring); metabolized to 2 active metabolites whose t1/2 are longer than parent. Ode is equipotent -> mode is more potent. Has aryloxypropanolamine pharmacophore; chiral carbon; r=s for na channel but s>r for beta blockade; s eliminated faster; hepatic metabolism; 5"hydroxypropafenone is just as strong of an na blocker. Addition of another sub is less selective adrenergic e ect on pm cells > increases said e ect; Miscellaneous greater (-) inotropic e ects -> stronger exacerbation of arrhythmias/higher likelihood of new ones.