PSYC 4430 Lecture Notes - Autism Spectrum, Tic Disorder, Dsm-5

10 Jun 2018
School
Department
Course
Professor

Chapter 13: Neurodevelopmental and Neurocognitive Disorders
1. Overview
a. Difference between normal and abnormal
i. Child’s age
ii. Child’s eiroet
b. Usually diagnosed in infancy, childhood, or adolescence
2. Communication and motor disorders
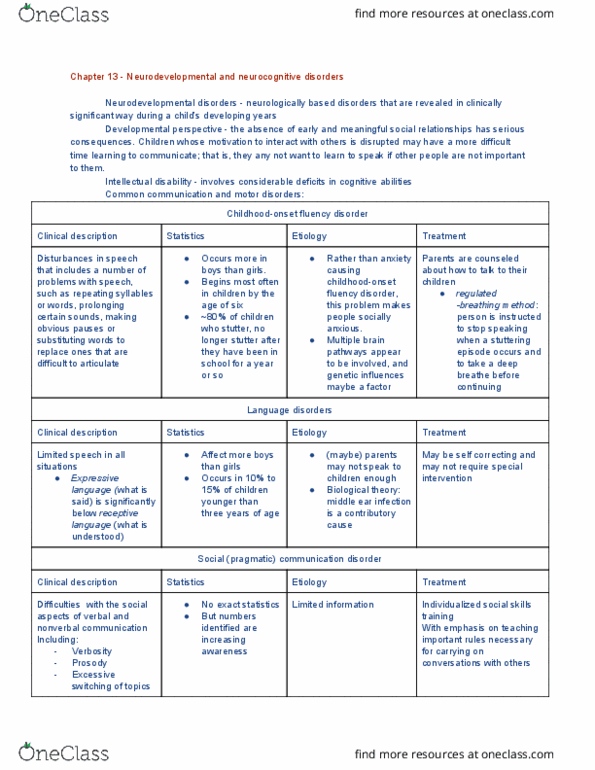
a. Childhood-onset fluency disorder (stuttering)
i. Sound/syllable repetition/prolongation; broken words; blocking and
pauses in speech; making substitutions for hard words; physical difficulty
with speech
ii. The disordered fluency impairs functioning in school, work, etc.
iii. Speech problems worsen in high-stress situations but are often absent
when the person is reading aloud, singing, or talking to a pet
iv. Often manifests by age 6, either suddenly (insidious onset) or gradually;
prognosis can be determined by the severity of the disorder at age 8
b. Language disorder (aka expressive language disorder)
i. Difficulty with expanding vocabulary with sentence structure (syntax,
grammar, and other sentence rules), and with discourse (forming and
connecting sentences to explain a topic of event)
ii. Deficits will appear in spoken, written, and/or gestured communication
iii. “ie there’s ot ofte faily history, the perso ay eoe adept at
not bringing attention to and compensating for his/her deficits
iv. He or she may prefer to only communicate with family members
v. Onset is usually around 4 years old and the disorder usually has a lifetime
course
c. Social (pragmatic) communication disorder
i. Difficulty adapting communication for different context; interrupting
others; not knowing how to use communication to interact
ii. Deficits are not because of language difficulty, cognitive problems, or low
intelligence
iii. People within the autism spectrum may have similar deficits, but with
additional problems with restricted/repetitive behavior, interests, or
activities
iv. Nor usually diagnosed until adolescence, when there are higher
expectations for social communication and complex interactions
d. Tourette’s disorder
i. Tic disorder
ii. Moth motor and vocal tics have been present; tics may come and go over
time but have to persist for over a year after onset
iii. Onset is before 18 years
iv. Tics may include profanity, sexual or obscene gestures, imitating
soeoe else’s oeets, repeatig oeself, or the last-yeard word,
phrase, or sound
find more resources at oneclass.com
find more resources at oneclass.com

3. Attention deficit hyperactivity disorder
a. Nature of ADHD
i. Inattention
ii. Hyperactivity/impulsivity
b. Onset is in childhood
c. There are factors that compensate for symptoms and may put off diagnosis
d. Types of ADHD
i. Predominantly inattentive presentation
1. Difficulty paying attention to detail/making careless mistakes
2. Difficulty sustaining attention in lectures, conversations, long
readings, and other tasks and activities
3. Difficulty following through with instructions/finishing homework,
chores, etc.
a. Dislikes/avoids such tasks
4. Often forgets important items and items necessary for such tasks
5. Easily distracted by extraneous stimuli
6. May forget tasks/appointments/assignments/etc.
ii. Predominantly hyperactive/impulsive presentation
1. Fidgeting
2. Abruptly leaves seat in setting where seating is expected
3. Running around/climbing in inappropriate settings (more
common for children; adolescents/adults may feel restless
instead)
4. Difficulty with quiet play or leisure activities
5. Difficulty being still for extended periods
6. Excessive talking
7. Blurting/interrupting
8. Diffiulty aitig for oe’s tur
iii. Combined presentation
iv. Other specified
v. Unspecified
e. Symptoms must be present before 12 years
f. Symptoms must be present in 2 or more settings
g. Symptoms may be milder/absent when:
i. Person is consistently rewarded for appropriate behavior
ii. Under dose supervision
iii. In a novel/new/fun setting
iv. Engaging in interesting/stimulating activities
h. Prevalence
i. Occurs in about %5 of children and 2.5% of adults in US
ii. Consistent across culture
iii. Female to male ratio is 2:1 for children and 1.6:1 for adults
i. Onset
find more resources at oneclass.com
find more resources at oneclass.com

i. Symptoms must be present before years, ut it’s hard to diagose
before 4 years
ii. Diagnosed because of discrepancies between patient and developmental
norms/intellectual capacity
j. Testing
i. WAIS-III or WISC
ii. Surveys administered to parents, teachers, employers, etc.
iii. Self-report surveys
k. Causes and associated factors
i. Chemical factors—usually a dopamine deficiency, but other
neurotransmitters may be resolved
ii. Genetic factors—the deficiency seems to be genetic (linked to the DAT1
gene)
iii. Environmental factors—low birth rate, maternal smoking during prenatal
period, toxins in food, negligent parenting, etc. have correlation to ADHD
iv. Neurological factors—smaller brain volume, inactivity of the frontal
cortex and basal ganglia, and abnormal frontal lobe development and
functioning
v. Temperamental factors—limited behavioral inhibition, negative
emotionality, thrill-seeking, etc. may predispose a child to ADHD
vi. Associated outcomes—people with ADHD are more likely to have poorer
school and occupational performance, are subject to bullying and low
self-esteem, and are more likely to develop conduct disorder and
subsequent antisocial personality disorder
l. Comorbidity
i. Oppositional defiant disorder
ii. Conduct disorder
iii. Disruptive mood dysregulation disorder
iv. Specific learning disorder
v. Anxiety disorder
vi. Major depressive disorders
vii. Intermittent explosive disorder (low impulse/rage control)
viii. Personality disorder
m. Psychosocial treatments and interventions
i. Educational assistance—extra time to take tests, standing up during tests
ii. Programs that reinforce appropriate behavior
iii. Educating parents about ADHD
n. Medical treatments and interventions
i. Stimulants: Ritalin, Adderall, Vyvanse
1. May act as dopamine agnosists for those with predominantly
inattentive presentation, giving them more energy and
diminishing symptoms
2. May act as dopamine antagonists for those with predominantly
hyperactive/impulsive presentation, calming them down
find more resources at oneclass.com
find more resources at oneclass.com